
The “Ornamental vaccinometry” It is a recent discipline but very topical in the media and, why fool ourselves, even among healthcare professionals. Its best known product is “Ornamental comparative vaccinometer”. That is, a television image or a printed table (like the one in the figure below) in which, always in large numbers, adorns a comment on the “efficacy” of vaccines against covid-19, usually accompanying some other detail about dose or temperature.
These “efficacy” figures are usually derived from phase III clinical trials of vaccines. Pfizer, Modern, AstraZeneca or from Janssen (Johnson & Johnson) still unpublished reports. But, contrary to what the media tend to say, they should not be interpreted as “protection” or “percentage of people protected” but as a reduction in relative risk (RRR) of becoming ill in the vaccinated compared to the unvaccinated.
Vaccine efficacy is “relative”
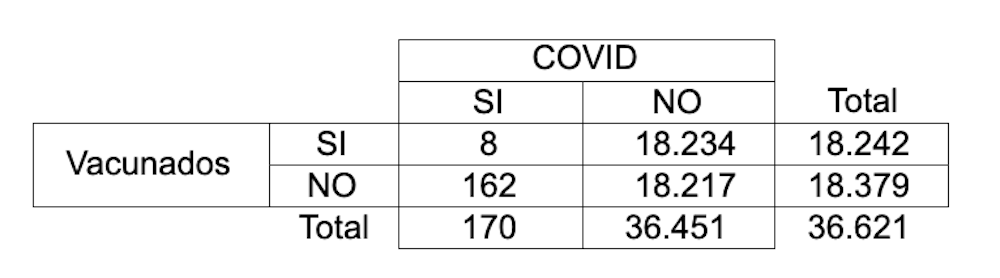
It is known that epidemiologists are addicted to 2×2 tables. The numbers below are from the Pfizer vaccine trial. They refer to vaccinated or unvaccinated patients, without prior serological or virological evidence of covid-19, who developed the disease (at least one symptom and CRP +) after at least 7 days from the second dose.
It is easy to deduce that 0.88% of the non-vaccinated (162 out of 18,217, 88 out of every 10,000) got sick compared to only 0.04% of those vaccinated (8 out of 18,242; 4 out of 10,000). The Absolute Risk Reduction (RAR) disease (0.88 – 0.04) was 0.84 percentage points. Or, put another way, 84 fewer cases per 10,000 vaccinated people (with the criteria and context of that particular study).
In relative terms, the Relative risk (RR) disease in vaccinated compared to non-vaccinated (0.04 / 0.88 = 0.05) is 5%. But sometimes epidemiologists prefer to express the inverse (1-RR) for highlight the RRR, the relative reduction of risk. Which in this case (1-0.05) offers the result of 95%, which is the one that appears in the vaccinometers.
In vaccine trials, we used to call RRR “vaccine efficacy”. In this specific study, it would indicate that we can expect a single person to become ill from covid-19 among those vaccinated for every 20 who become ill among those who are not vaccinated.
A “vaccine efficacy” of 50%, the minimum required by the WHO for the commercialization of vaccines, would indicate that only one person becomes ill among those vaccinated for every two who contract the disease in those who are not vaccinated.
Necessary number of people to vaccinate to avoid a case of covid-19
“Vaccine efficacy” is a parameter relative. If in the previous study the incidence had been 100 times lower (4 and 88 cases per 1,000,000 vaccinated or unvaccinated people, instead of per 10,000), the “vaccine efficacy” would still be 95%, but its population impact it would be very different. To assess this aspect, epidemiologists use a parameter with absolute numbers: the number of people we need to vaccinate to avoid a case (number needed to treat or NNT).
A recent study showed these NNTs for the three vaccines currently authorized in the EU:
Not without surprise, the seemingly least “effective” vaccine is the one that prevents the most cases of covid-19. The fact is that the NNT, a much more important and interpretable parameter than the RRR, depends above all on the absolute (not relative) difference in risks. And this – despite the misinformation of the vaccinometers – was much higher in the AstraZeneca trial.
Pears, apples and clinical trials
There is no randomized clinical trial that has compared the different vaccines with each other. And the different trials have been carried out in different populations, in different countries with different incidences and different circulating variants, using different criteria to define what is a case of covid-19, with different comparators and with different follow-up times. And this means, plain and simple, that your efficacy results (or your NNT) cannot be compared. It would be like comparing pears and apples.
For example, the Astra-Zeneca and Janssen trials recruited many patients in Brazil and South Africa, two countries with wide circulation of variants with the E484K mutation that escapes, at least partially, the action of antibodies and where less efficiency could be expected. In fact, the Janssen vaccine offered better efficacy results in the United States than in South Africa or South America.
Not only that. In addition, the incidence of covid-19 (understood as the proportion of cases in the unvaccinated) during the field work of the trials varied significantly between studies. There were 88 cases per 10,000 among the Pfizer trials, and 296 at AstraZeneca. The characteristics of the populations also varied. For example, the one at AstraZeneca recruited a large proportion of healthcare personnel to speed up the trial because of their increased exposure.
Another detail to take into account is that very different definitions of “case” were also used. For example, the Pfizer trial required that patients have no serological or virological evidence of infection until 7 days after the 2nd dose, at which point they began to be counted as CoViD cases. For its part, Moderna’s demanded evidence of not being infected until the moment of the 1st dose, but began to count the cases 14 days after the second.
On the other hand, all the trials used placebo in the control groups except that of AstraZeneca, which used another vaccine (meningococcal). And that makes it possible that the patients in the control group had some protection due to the action of heterologous (“crossed”) immunity mechanisms.
We cannot affirm that vaccines are the same, but neither that they are different
There are many things we still need to know about vaccines. Among others, its comparative effectiveness, the duration of immunity, the real effectiveness against new variants and its side effects in long-term follow-up.
What we do know is that they all manage to reduce severe cases of covid-19. All the trials have shown an excellent effectiveness profile against covid-19 hospitalization. And also the studies with real life data in Israel, Scotland The England. In the latter two, with a high and very similar effectiveness for the Pfizer and AstraZeneca vaccines with a single dose.
On the other hand, population vaccination – with any vaccine authorized in the EU – has an important advantage over clinical trials: herd immunity. Each vaccinated person increases the effectiveness of the vaccine in the population as a whole. Each person who is vaccinated increases protection for all people.
With current information we cannot say that any vaccine is superior to another. Although this does not mean that they are equal, because we do not have comparative non-inferiority studies that allow us to equate them.
Television “vaccinometry”, which confuses “vaccine efficacy” in different trials with the superiority or inferiority of one or another vaccine in the real world, is a form of ignorance that damages the vaccine campaign and puts people at risk. The false belief that there are first and second vaccines is spreading among the population. It is not only “disinformative”, it is harmful.
–


{kind=link}