Low Grip Strength Not a Reliable Predictor of Prostate Cancer in Older Men
Recent clinical analysis indicates that low grip strength should not be utilized as an independent clinical predictor for prostate cancer risk in aging male populations. While physical frailty markers are often associated with systemic health, researchers have determined that muscle strength metrics lack the diagnostic specificity required to serve as a standalone screening tool for prostatic malignancies.
Key Clinical Takeaways:
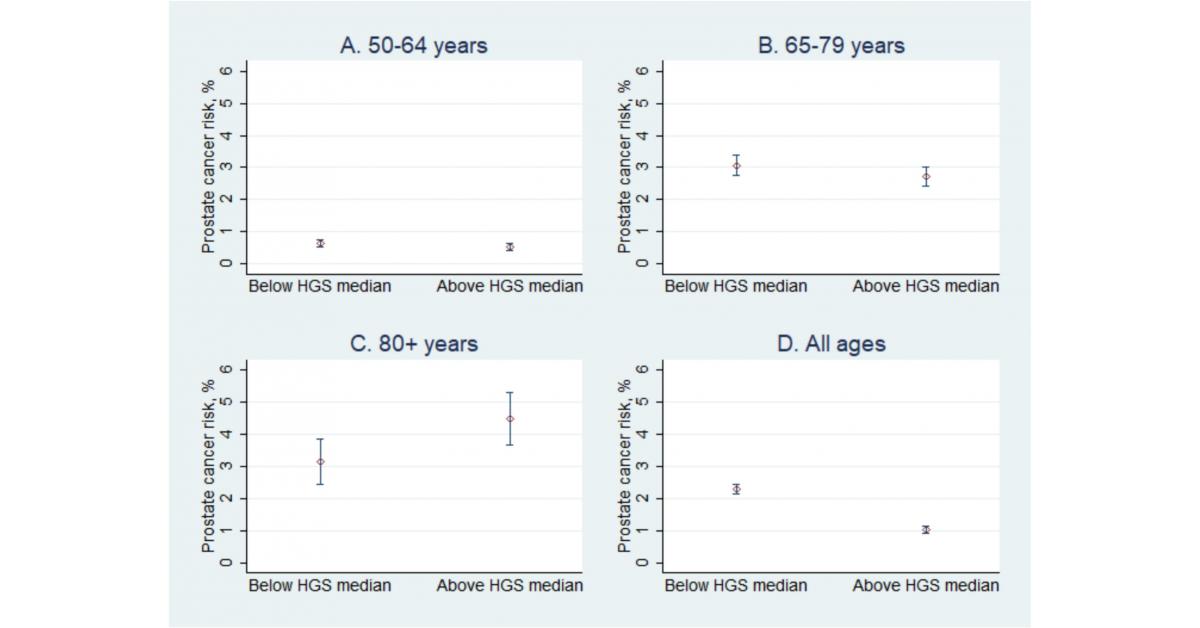
- Grip strength, while a useful indicator of general sarcopenia and functional decline, does not demonstrate a statistically significant correlation with prostate cancer incidence.
- Clinical guidelines maintain that prostate-specific antigen (PSA) testing and digital rectal examinations remain the standard of care for early detection.
- Patients should prioritize comprehensive geriatric assessments and established oncological screening protocols over isolated physical performance metrics when evaluating cancer risk.
The Diagnostic Limitations of Physical Performance Metrics
In the field of geriatric medicine, clinicians frequently employ grip strength as a proxy for physical vitality and overall morbidity risk. However, the application of this metric to oncological screening remains scientifically unsupported. According to recent findings, relying on grip strength as a predictor for prostate cancer introduces a risk of diagnostic over-reliance on non-specific biomarkers. This approach risks misclassifying patients or providing a false sense of security regarding their oncological status.

The pathogenesis of prostate cancer is multifactorial, involving complex genetic, hormonal, and environmental interactions that are distinct from the biological mechanisms governing skeletal muscle maintenance. For patients concerned about their risk profile, it is essential to engage with board-certified urologists who utilize evidence-based diagnostic pathways rather than proxy metrics.
Standard of Care vs. Emerging Biomarkers
The medical community emphasizes that the current gold standard for prostate cancer detection relies on a combination of PSA levels, imaging studies, and biopsy when indicated. Research published in journals such as PubMed consistently highlights that while physical activity is beneficial for general health, it does not mitigate the necessity for traditional screening.
Physicians must distinguish between sarcopenia-related frailty and oncological risk. As noted in longitudinal studies, the lack of a direct causal mechanism between handgrip power and prostate cell mutation renders the former an unreliable surrogate marker. For those navigating the complexities of prostate health, consulting with specialized diagnostic centers ensures that patients receive testing that aligns with current clinical consensus rather than anecdotal or correlative observations.
Clinical Logic and Patient Triage
When clinicians encounter patients presenting with concerns regarding cancer risk, the priority remains the mitigation of diagnostic delays. The current literature suggests that focusing on irrelevant physical markers can distract from the necessary, time-sensitive screenings required for early intervention. For healthcare providers, the objective is to streamline the referral process to ensure that at-risk individuals receive timely PSA testing and, where appropriate, referral to oncology specialists.
The integration of digital health records and standardized screening protocols is vital to maintaining high-quality outcomes. For those requiring a second opinion or a comprehensive risk assessment, accessing vetted medical specialists serves as the most effective strategy to avoid diagnostic bottlenecks. By adhering to established guidelines, practitioners can better manage patient expectations and reduce the morbidity associated with late-stage diagnosis.
Future Trajectories in Oncological Assessment
As the medical field continues to refine its approach to precision medicine, the emphasis will remain on genomic and molecular diagnostics rather than broad physical performance indices. The rejection of grip strength as an independent predictor reflects a move toward higher clinical specificity. Future research is expected to continue focusing on the validation of novel liquid biopsies and advanced imaging modalities that offer clearer insight into prostatic health.
For patients and providers alike, the focus must remain on proven screening methodologies. Engaging with the broader medical community to stay updated on these protocols is essential for anyone involved in managing long-term prostate health. Those seeking guidance on modern diagnostic standards should consult with qualified healthcare practitioners who prioritize evidence-based medicine in every clinical encounter.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.