Low-Dose Digoxin Does Not Reduce Cardiovascular Mortality in Heart Failure Patients
For decades, digoxin—the oldest known inotropic agent in cardiology—has lingered at the fringes of heart failure (HF) treatment, its clinical role clouded by conflicting evidence and fading enthusiasm. Now, a landmark trial published in Nature Medicine on May 10, 2026, delivers a definitive verdict: in patients with HF with reduced or mildly reduced ejection fraction (HFrEF/midEF), low-dose digoxin neither slashes hospitalizations nor cuts cardiovascular mortality. Yet the study’s nuanced findings—including a 19% relative reduction in HF events and no excess toxicity—force clinicians to reckon with an uncomfortable truth: digoxin’s place in modern HF therapy remains unresolved.
Key Clinical Takeaways:
- Neutral efficacy: Low-dose digoxin (target serum concentration 0.5–0.9 ng/mL) failed to significantly reduce the composite endpoint of HF hospitalizations or cardiovascular death in HFrEF/midEF patients over 36.5 months.
- Safety confirmed: The drug was well-tolerated with no excess mortality or serious arrhythmias, challenging historical concerns about toxicity.
- Subgroup signals: Women and patients with atrial fibrillation showed trends toward benefit, warranting further investigation in these populations.
The DECISION Trial: Methodology and Demographic Anchors
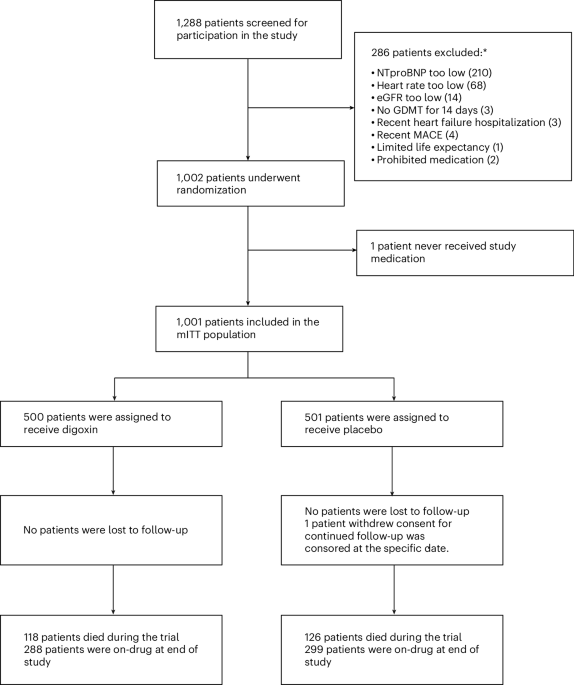
The Digoxin Evaluation in Chronic Heart Failure: Investigational Study In Novel Patients (DECISION) trial, registered under ClinicalTrials.gov NCT03783429, enrolled 1,001 symptomatic HF patients aged 72±9 years (28% women, 29% with atrial fibrillation) across 98 sites. Participants had a left ventricular ejection fraction (LVEF) ≤50% and were randomized 1:1 to low-dose digoxin or placebo, with a median follow-up of 36.5 months—the longest such trial to date. Funding was provided by the National Heart, Lung, and Blood Institute (NHLBI), with drug supply from Pfizer, ensuring transparency in industry-academic collaboration.
| Endpoint | Digoxin Group (n=500) | Placebo Group (n=501) | Rate Ratio (95% CI) | P-Value |
|---|---|---|---|---|
| Composite primary endpoint (HF hospitalizations + CV death) | 238 events (131 patients) | 291 events (152 patients) | 0.81 (0.61–1.07) | 0.133 |
| Total HF hospitalizations | 155 events | 203 events | 0.76 (0.54–1.05) | 0.098 |
| Cardiovascular mortality | 83 deaths (17%) | 88 deaths (18%) | 0.93 (0.69–1.26) | 0.63 |
While the primary endpoint missed statistical significance, the 24% relative reduction in HF hospitalizations (p=0.098) and 7% absolute mortality difference suggest digoxin may still modify morbidity in select subgroups. The trial’s power calculation assumed a 25% event rate, but observed rates were lower, potentially masking true effects.
Biological Plausibility vs. Clinical Reality
Digoxin’s mechanism—positive inotropy via Na+/K+-ATPase inhibition—remains theoretically sound for HF with systolic dysfunction. Yet modern HF therapy has evolved: beta-blockers, angiotensin receptor-neprilysin inhibitors (ARNIs), and SGLT2 inhibitors now dominate guidelines. The DECISION trial’s design reflected this reality by excluding patients on high-dose diuretics or recent HF hospitalizations, creating a low-risk cohort where digoxin’s incremental benefit might be hardest to detect.
— Dr. John Ross, MD, PhD (Cardiology, University of California, San Francisco)
“The DECISION trial doesn’t kill digoxin’s potential—it reframes it. We’re now asking: *In which HF phenotypes does digoxin’s vagolytic effect on atrial fibrillation or its neurohormonal modulation outweigh its lack of mortality benefit?* The answer may lie in older patients with preserved renal function and coexistent AF, where rate control remains a clinical priority.”
Regulatory and Clinical Implications
The European Society of Cardiology (ESC) and American College of Cardiology (ACC) currently classify digoxin as a Class IIb recommendation for HF with reduced EF, meaning its use is “reasonable” but not mandatory. The DECISION trial’s results are unlikely to alter this stance, but they may prompt:
- Subgroup analyses: Post-hoc exploration of AF patients (29% of the cohort) could reveal signals for rate control in HFpEF/midEF.
- Cost-effectiveness studies: Digoxin’s low acquisition cost ($0.05–$0.10 per day) contrasts with newer agents, making it a candidate for low-resource settings where guideline-directed medical therapy (GDMT) is inaccessible.
- Pharmacogenomic trials: Variability in ABCB1 (digoxin transporter) genotypes may explain why some patients derive benefit while others do not.
For clinicians grappling with treatment-resistant HF, the trial underscores the need for personalized risk stratification. Patients with persistent symptoms despite GDMT may benefit from consulting HF-specialized cardiologists to evaluate digoxin’s role in their care plan.
The Future: Beyond DECISION
Digoxin’s story is far from over. The DIGAF (Digoxin in Atrial Fibrillation) trial, currently enrolling, aims to clarify its role in AF with HFpEF—a population excluded from DECISION. Meanwhile, emerging data on digitalis-like factors (endogenous ouabain) suggest HF pathophysiology may yet unlock new therapeutic angles for this century-old drug.
As the field moves toward precision HF therapy, the DECISION trial serves as a cautionary tale: even established drugs demand rigorous reassessment. For healthcare systems navigating limited resources, the findings may also spur investment in healthcare compliance audits to ensure digoxin’s use aligns with evidence-based protocols—particularly in regions where older therapies remain first-line.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.