
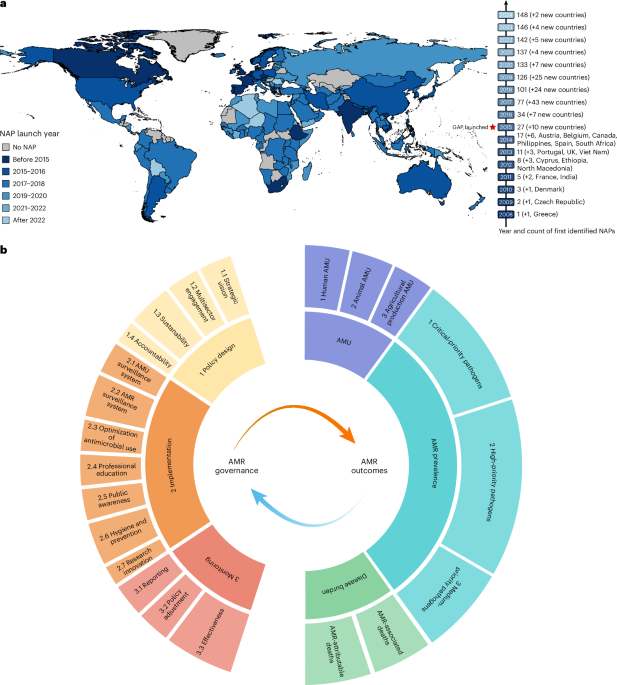
A global assessment of national strategies to combat antimicrobial resistance (AMR) reveals uneven progress and highlights the critical necessitate for improved governance, according to research published January 7 in Global Health. The study, spanning 2000-2021 across 193 countries, found that while many nations have adopted national action plans (NAPs) to address the growing threat of drug-resistant infections, the effectiveness of these plans varies significantly.
Researchers, led by Archie Drake, an independent consultant based in Tanzania, analyzed national AMR policy documents, data from the Tracking AMR Country Self-Assessment Survey (TrACSS) and information from the United Nations Children’s Fund (UNICEF) and the Global AMR R&D Hub. The study constructed an index to characterize national AMR governance across multiple domains, including policy design, implementation, and monitoring. Data collection was completed in November 2024.
The analysis revealed that 269 out of 832 national policy documents were retained for in-depth analysis – 200 NAPs and 69 related policy or legal documents. Native-language NAPs, totaling 118 in 39 languages, were translated using Google Translate. Four researchers independently reviewed these documents, rating governance indicators based on Cochrane Systematic Review standards, with discrepancies resolved through discussion or arbitration.
The study linked AMR governance to three key outcomes: antimicrobial use (AMU), AMR prevalence, and disease burden. Researchers found that improvements in governance were not consistently associated with improvements in AMR-related outcomes, suggesting that simply having a plan in place is not enough. The effectiveness of governance appears to hinge on robust implementation and ongoing monitoring.
The research identified significant regional disparities. The WHO regional characterization proved more effective than alternative schemes in capturing heterogeneity across regions, particularly in Asia, where the WHO distinguishes between the Eastern Mediterranean, South-East Asia, and Western Pacific regions, reflecting differing AMR governance trajectories.
To address data gaps, researchers employed imputation strategies for missing AMU data. Missing human AMU values for 2019-2021 were projected using country-specific autoregressive integrated moving average (ARIMA) models. Animal AMU time series for 2000-2021 were constructed by backcasting and forecasting from observed 2020 values using country-specific annual percentage changes (APCs) derived from each country’s sociodemographic index (SDI) trajectory.
The study’s governance framework was developed through a Delphi consultation involving an international expert panel of 38 individuals from diverse fields, including clinical medicine, veterinary medicine, and environmental science. Experts refined the framework through virtual roundtable discussions and two rounds of Delphi surveys, generating a draft indicator list based on international policy frameworks like the WHO Global Action Plan on AMR. Indicators were retained for analysis only if they achieved a mean importance score of 3.5 or higher and a coefficient of variation of 0.25 or lower.
Researchers used a combined subjective-objective weighting strategy to derive indicator weights for the AMR governance index, AMU, and AMR prevalence scores. Subjective weights were obtained through a Delphi-based Analytic Hierarchy Process (AHP), while objective weights were computed using the entropy method. These were integrated using a deviation-maximization method to balance expert judgment and data-driven variability.
Using a difference-in-differences (DID) framework, the study examined the association between NAP adoption and AMR-related outcomes. Results indicated that the impact of NAP adoption varied, highlighting the importance of considering staggered policy implementation and heterogeneous treatment effects. Joinpoint regression analysis identified statistically significant inflection points in temporal trends of AMR prevalence scores, with some changes coinciding with the 2015 release of the WHO GAP on AMR.
Latent class growth modeling identified distinct trajectories of AMR prevalence changes post-GAP, revealing that some countries demonstrated substantial improvements while others experienced continued increases. Analysis of 17 countries that adopted NAPs before the 2015 GAP release and 29 countries showing the greatest improvements in AMR prevalence revealed governance factors associated with positive outcomes. The study is ongoing, with researchers continuing to analyze the complex interplay between governance, policy, and AMR-related outcomes.