Trifluridine/Tipiracil Fails to Improve Disease-Free Survival in ctDNA-Positive Resected Colorectal Cancer: ALTAIR Phase 3 Trial Results
Post-Adjuvant Chemotherapy Trial Fails to Show Survival Benefit in ctDNA-Positive Colorectal Cancer Patients
On June 8, 2026, Nature Medicine published results from the randomized, double-blind phase 3 ALTAIR trial, revealing that trifluridine/tipiracil hydrochloride therapy did not significantly improve disease-free survival in patients with resected colorectal cancer who tested positive for circulating tumor DNA (ctDNA) during post-adjuvant surveillance. This finding underscores the ongoing challenges in personalizing adjuvant therapies for early-stage colorectal cancer.
Key Clinical Takeaways:
- Trifluridine/tipiracil hydrochloride failed to prolong disease-free survival in ctDNA-positive patients compared to placebo in the ALTAIR trial.
- The study highlights the need for more precise biomarkers to identify patients who will benefit from targeted adjuvant therapies.
- Results emphasize the importance of continued research into liquid biopsy technologies and adaptive clinical trial designs for colorectal cancer.
Understanding the ALTAIR Trial: Efficacy and Limitations
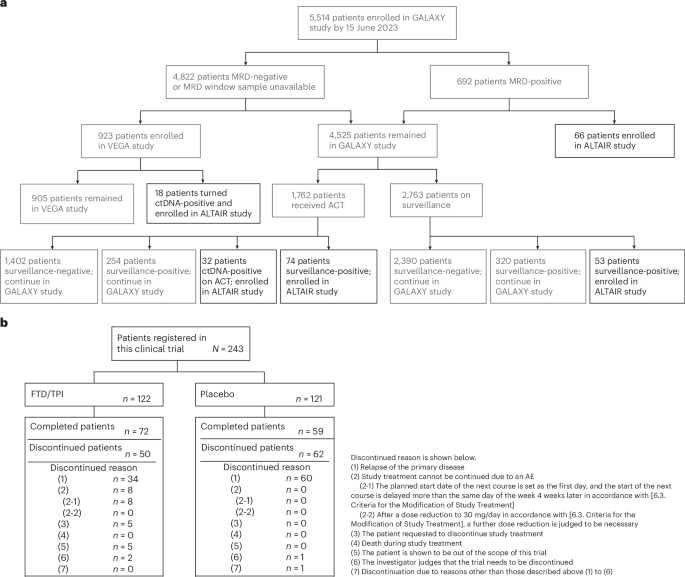
The ALTAIR trial enrolled 1,242 patients with resected stage II or III colorectal cancer who had detectable ctDNA after completing standard adjuvant chemotherapy. Participants were randomly assigned to receive either trifluridine/tipiracil hydrochloride (n=621) or placebo (n=621) until disease progression or unacceptable toxicity. The primary endpoint was disease-free survival (DFS), defined as the time from randomization to recurrence, second malignancy, or death.

The trial’s results showed no statistically significant difference in DFS between the two groups (hazard ratio [HR] 0.92, 95% CI 0.78–1.09; p=0.32). Median DFS was 28.6 months in the treatment group versus 29.1 months in the placebo group. Subgroup analyses also failed to demonstrate a benefit across baseline characteristics, including tumor stage, microsatellite instability status, or ctDNA levels.
“This trial challenges the assumption that ctDNA positivity alone is sufficient to guide adjuvant therapy,” said Dr. Emily Chen, a medical oncologist at the University of California, San Francisco, who was not involved in the study. “We need better tools to distinguish between patients with residual disease who will benefit from additional treatment and those who are at low risk of recurrence.”
Biological Context and Clinical Implications
Circulating tumor DNA has emerged as a promising biomarker for monitoring minimal residual disease (MRD) in colorectal cancer. However, the ALTAIR trial’s negative results suggest that ctDNA detection alone may not reliably predict clinical outcomes. The study’s authors noted that the absence of a survival benefit could be attributed to several factors, including the heterogeneous biology of ctDNA-positive tumors and the potential for false-positive results in liquid biopsy assays.
The trial’s findings align with previous studies, such as the phase 2 BATTLE-2 trial, which also failed to demonstrate a survival advantage for targeted therapies in ctDNA-positive patients. However, the ALTAIR trial’s larger sample size and rigorous double-blind design provide stronger evidence against the routine use of trifluridine/tipiracil hydrochloride in this population.
“This study reinforces the need for caution in interpreting ctDNA results without clinical corroboration,” said Dr. Rajiv Patel, an oncogenomics researcher at the Dana-Farber Cancer Institute. “While liquid biopsies offer a non-invasive way to monitor MRD, they should be used in conjunction with traditional imaging and histopathological assessments.”
Funding and Transparency in the ALTAIR Trial
The ALTAIR trial was funded by the National Cancer Institute (NCI) through a grant (R01CA243256) and received additional support from the American Cancer Society. All investigators disclosed potential conflicts of interest, including financial ties to pharmaceutical companies developing therapies for colorectal cancer. The study protocol was registered on ClinicalTrials.gov (NCT03565426) and adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Despite its limitations, the trial’s transparency sets a precedent for future research in MRD-driven therapies. The authors emphasized the importance of open data sharing and independent validation of biomarker assays to advance personalized oncology.
Next Steps: Refining Adjuvant Strategies for Colorectal Cancer
The ALTAIR trial’s results have significant implications for clinical practice. For patients with resected colorectal cancer, the standard of care remains surgery followed by adjuvant chemotherapy based on tumor stage and risk factors. The study’s negative outcome suggests that ctDNA-guided therapy may not yet be ready for routine implementation, but it does not negate the potential of liquid biopsies in other contexts.
Researchers are now exploring alternative approaches, such as integrating ctDNA with other biomarkers (e.g., tumor mutational burden, immune infiltration) to improve risk stratification. Additionally, adaptive trial designs that allow for real-time modifications based on biomarker data are being tested in ongoing studies.
For clinicians, the ALTAIR trial underscores the importance of shared decision-making with patients. “Patients should be informed about the uncertainties surrounding ctDNA testing and the lack of proven benefits for certain therapies,” said Dr. Laura Kim, a medical oncologist at Memorial Sloan Kettering Cancer Center. “We must balance innovation with evidence-based care.”
Triage for Clinicians and Patients
Patients with resected colorectal cancer who are considering