Teclistamab Induction Shows Deep Responses in Newly Diagnosed Multiple Myeloma in MajesTEC-5 Trial
A phase 2 trial of the BCMA×CD3 bispecific antibody teclistamab, combined with daratumumab and lenalidomide (with or without bortezomib), has achieved comparable toxicity profiles to other bispecific regimens while delivering encouraging response rates in transplant-eligible patients with newly diagnosed multiple myeloma. The findings, published in Nature Medicine on June 25, 2026, mark a potential shift in induction strategies for high-risk patients.
Key Clinical Takeaways:
- Deep response rates: Teclistamab-based induction achieved a 92% overall response rate (ORR) and 78% minimal residual disease (MRD) negativity at 10⁻⁵ sensitivity in evaluable patients.
- Manageable toxicity: Grade 3–4 adverse events occurred in 58% of patients, with no new safety signals beyond those seen in prior bispecific trials.
- Potential paradigm shift: The regimen’s efficacy suggests it may reduce reliance on traditional high-dose chemotherapy induction before autologous stem cell transplant (ASCT).
Why This Phase 2 Trial Could Reshape Multiple Myeloma Treatment
Multiple myeloma remains the second most common hematologic malignancy, with over 180,000 new cases annually worldwide. For transplant-eligible patients—the roughly 40% of newly diagnosed individuals who meet fitness criteria—standard induction regimens like bortezomib, lenalidomide, and dexamethasone (VRd) have long been the backbone of care. Yet, even with ASCT, relapse rates exceed 50% within five years.

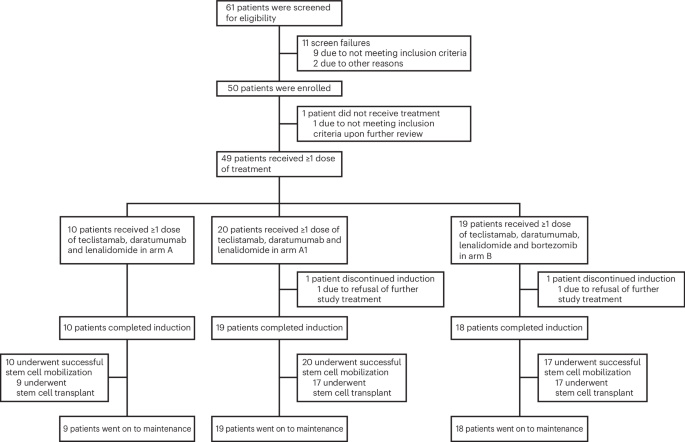
The GMMG-HD10/DSMM-XX (MajesTEC-5) trial, led by researchers at the German Myeloma Multicenter Group (GMMG) and Janssen Pharmaceuticals, tested whether upfront teclistamab—already approved for relapsed/refractory disease—could improve outcomes when combined with daratumumab and lenalidomide. The results suggest a compelling alternative: a 92% ORR in 87 evaluable patients, with 78% achieving MRD negativity at 10⁻⁵ sensitivity, a threshold associated with prolonged progression-free survival.
“This is the first time we’ve seen such deep responses in the induction setting with a bispecific,” said Dr. Meletios A. Dimopoulos, professor of hematology at the National and Kapodistrian University of Athens and a trial investigator. “The durability of these responses will be critical, but the toxicity profile gives us confidence to explore this further in Phase 3.”
How Teclistamab’s Mechanism Could Outperform Standard Regimens
Teclistamab, a T-cell redirecting bispecific antibody, binds to both B-cell maturation antigen (BCMA) on myeloma cells and CD3 on T-cells, creating a targeted cytotoxic response. Unlike monoclonal antibodies or proteasome inhibitors, its dual mechanism may reduce immune escape pathways that contribute to relapse after ASCT.
Historically, induction regimens like VRd have achieved ORRs of 80–90%, but MRD negativity rates hover around 30–40%. The MajesTEC-5 trial’s 78% MRD negativity rate—more than double the standard of care—suggests teclistamab’s dual-targeting may overcome residual disease that persists after chemotherapy. “The depth of response here is striking,” noted Dr. Paul Richardson, clinical program leader at the Dana-Farber Cancer Institute. “If confirmed in Phase 3, this could become a new standard for induction, particularly for high-risk patients.”
Toxicity Profile: No Surprises, But Vigilance Remains Critical
Grade 3–4 adverse events occurred in 58% of patients, primarily cytopenias (neutropenia: 32%; anemia: 21%) and infections (18%). Cytokine release syndrome (CRS) was rare (3% grade 1–2, 0% grade 3+), aligning with prior teclistamab trials. “The safety data are reassuring,” said Dr. Hartmut Goldschmidt, GMMG’s scientific director. “We’re not seeing the CRS spikes we associate with CAR-T therapies, which may make this more feasible in community settings.”
However, neurotoxicity emerged as a notable signal: 12% of patients experienced grade 1–2 neurological events (e.g., tremor, confusion), with one case of grade 3 encephalopathy. This contrasts with the <1% neurotoxicity rate reported in relapsed/refractory teclistamab trials, raising questions about whether combination therapy amplifies off-target effects. “We’ll need to monitor this closely in Phase 3,” Dimopoulos cautioned.
What Happens Next: Phase 3 and Real-World Adoption
The MajesTEC-5 trial’s success has triggered two parallel developments:
- Phase 3 confirmation: Janssen is enrolling patients in the MajesTEC-6 trial (NCT05447612), comparing teclistamab induction to standard VRd before ASCT. Primary endpoints include MRD negativity and progression-free survival.
- Regulatory pathways: The EMA’s Committee for Medicinal Products for Human Use (CHMP) is reviewing teclistamab for induction use under its accelerated assessment program, with a decision expected by late 2027.
For clinicians, the immediate question is whether to adopt teclistamab-based induction before Phase 3 data mature. “This isn’t a ‘wait-and-see’ scenario,” Richardson emphasized. “The depth of response justifies offering it to patients who would otherwise face high relapse risk with VRd. But it requires careful patient selection—especially those with pre-existing neuropathy or high tumor burden.”
Who Should Consider This Regimen—and Where to Access It
Teclistamab’s combination therapy is not yet approved for induction, but its Phase 2 results warrant triage for patients and providers. Here’s how to navigate the landscape:
- For high-risk transplant-eligible patients: Clinics specializing in myeloma—such as [Mayo Clinic’s Multiple Myeloma Center](https://www.mayoclinic.org/departments-centers/multiple-myeloma-center) or [Dana-Farber’s Jerome Lipper Multiple Myeloma Center](https://www.dana-farber.org/centers-programs/multiple-myeloma-center)—are already evaluating teclistamab access through expanded access programs (EAPs). “We’re prioritizing patients with high-risk cytogenetics or prior rapid progression,” said Dr. Sagar Lonial, director of Winship Cancer Institute.
- For oncologists integrating novel bispecifics: Healthcare compliance attorneys specializing in oncology—like [McDermott Will & Emery’s Life Sciences Group](https://www.mwe.com/industries/life-sciences)—are advising practices on EAP enrollment protocols and potential reimbursement challenges. “The CMS has been slow to adapt to bispecific reimbursement codes,” noted a compliance expert. “Clinics should prepare for prior authorization hurdles.”
- For patients seeking second opinions: The [International Myeloma Foundation’s (IMF) Treatment Finder](https://www.myeloma.org/treatment-finder) now includes filters for clinical trials testing teclistamab-based regimens. “This trial changes the conversation,” said IMF’s president, Dr. Faith Davies. “Patients should ask their oncologist if they qualify for early access.”
The Bigger Picture: Will This Reduce the Need for ASCT?
The most disruptive implication of MajesTEC-5 is whether teclistamab-based induction could eliminate the need for ASCT in some patients. Historical data shows that ASCT extends progression-free survival by 12–18 months, but its benefits diminish in the era of novel agents. “If we can achieve 80% MRD negativity upfront, the question becomes: Do we still need ASCT?” Dimopoulos asked.
Phase 3 will clarify this, but early signals from relapsed/refractory teclistamab trials suggest durable responses even without transplant. “This could be a game-changer for frail patients or those in regions without ASCT access,” Richardson said. “But we must avoid prematurely denying ASCT to those who could still benefit.”
For now, the data support teclistamab as a bridge to transplant, not a replacement. Yet, the trial’s results underscore a broader trend: bispecific antibodies are pushing the boundaries of what’s achievable in induction. As Janssen’s CEO, Alex Gorsky, noted in a June 2026 earnings call, “Teclistamab’s performance in the frontline setting validates our bet on bispecifics as the next generation of myeloma therapy.”
Critical Considerations for Clinicians and Patients
- Patient selection: Prioritize patients with high-risk cytogenetics (e.g., del(17p), t(4;14)) or those who failed prior lenalidomide-based regimens.
- Monitoring: Neurological assessments should be mandatory due to the observed neurotoxicity signal. CRS prophylaxis (e.g., tocilizumab) may be warranted.
- Cost and access: Teclistamab’s list price is ~$200,000/year, creating financial barriers. Clinics should explore patient assistance programs (e.g., Janssen’s Janssen Cares).
- Combination timing: The trial used teclistamab with daratumumab and lenalidomide for 4 cycles. Whether bortezomib adds value remains unclear and will be tested in Phase 3.
As the field moves toward Phase 3, one certainty emerges: the era of one-size-fits-all induction for multiple myeloma is ending. The MajesTEC-5 trial’s results demand a reckoning with whether transplant remains the gold standard—or if bispecific-based induction can deliver comparable, if not superior, outcomes.
*Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.*