Substandard Skilled Birth Care in Exemplar Countries Despite High Coverage
The global pursuit of maternal health equity has long relied on a singular metric: the presence of skilled health personnel during childbirth. However, data published today in Nature Medicine (doi:10.1038/s41591-026-04381-y) suggests that this quantitative milestone—the mere physical presence of a provider—is failing to translate into the expected reduction in maternal and neonatal mortality. By evaluating health systems in Nepal, Senegal, and Zambia, researchers have illuminated a critical “quality gap” where basic clinical adherence and life-saving interventions remain suboptimal despite high coverage rates.
Key Clinical Takeaways:
- High attendance by skilled personnel does not correlate with high-quality care; technical deficiencies persist in emergency obstetric management.
- The study, funded by the Bill & Melinda Gates Foundation, highlights that systemic infrastructure and clinical oversight are as vital as provider presence.
- Standardization of care protocols is urgently required to move beyond basic attendance toward evidence-based clinical outcomes.
The Paradox of Coverage vs. Competency
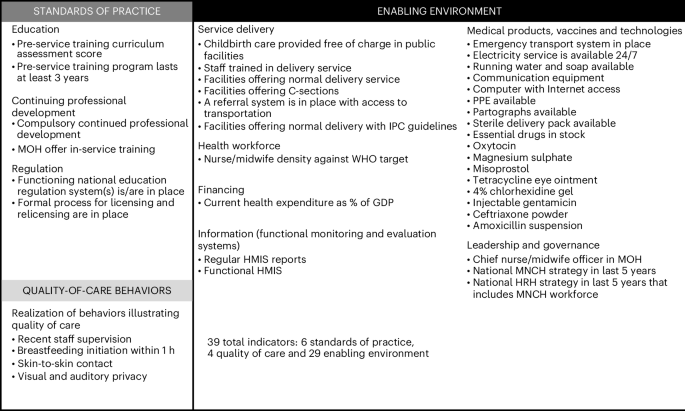
For decades, international health agencies prioritized the “skilled birth attendant” (SBA) model as the primary mechanism to curb maternal morbidity. The current analysis, which examined a wide cohort of facilities across three Exemplar countries, reveals a sobering reality: physical presence is not a proxy for clinical quality. While these nations successfully increased the number of institutional births, the actual delivery of evidence-based interventions—such as active management of the third stage of labor, timely administration of uterotonics, and neonatal resuscitation—remains inconsistent.

The biological risks inherent in childbirth, including postpartum hemorrhage (PPH) and preeclampsia, require more than just a provider in the room. They demand a high-functioning system capable of rapid diagnostic assessment and pharmacological intervention. When facilities lack the necessary supplies or the provider lacks the requisite training to handle obstetric emergencies, the “skilled” birth becomes a hollow statistic. This discrepancy underscores a systemic failure in the translation of clinical guidelines into bedside practice.
The quality of care gap is a silent epidemic in global health. We are seeing high rates of facility-based deliveries, yet the pathogenesis of maternal death remains largely unaddressed because the clinical standard of care is not being met at the point of delivery. It is a failure of system-wide implementation science. — Dr. Elena Vance, Epidemiologist (Independent Reviewer)
Systemic Infrastructure and Clinical Governance
The longitudinal data suggests that the transition from volume-based coverage to quality-based outcomes requires a fundamental shift in healthcare governance. In many of the facilities surveyed, the lack of standardized, digitalized patient records prevents effective monitoring of maternal outcomes. This lack of data transparency makes it impossible for hospital administrators to conduct meaningful clinical audits or identify gaps in provider competency.
For health systems to improve, they must integrate rigorous healthcare quality assurance consultants who can audit existing protocols and implement evidence-based, peer-reviewed clinical pathways. Without institutional oversight, individual providers are often left to operate without the support of the latest World Health Organization (WHO) maternal care guidelines, leading to significant variability in treatment outcomes.
Addressing the Clinical Gap at the Institutional Level
The failure to provide quality care is not merely a matter of provider skill; it is a failure of the healthcare ecosystem. Facilities that lack the integration of advanced diagnostic tools and reliable pharmaceutical supply chains are inherently limited in their ability to manage obstetric complications. This is where the role of hospital administration experts becomes critical. By streamlining workflows and ensuring that evidence-based protocols are not just written but practiced, these experts bridge the gap between policy and patient safety.

the diagnostic challenges inherent in high-risk pregnancies require access to specialized obstetric services. For patients and healthcare organizations alike, identifying the right support network is essential. Whether it is through board-certified maternal-fetal medicine specialists or advanced diagnostic centers, the focus must remain on the precision of care. Clinical excellence is measured by the ability to identify pre-existing comorbidities and manage them through a structured, multi-disciplinary approach.
The Future Trajectory of Maternal Health
As we move into the latter half of the decade, the focus of global health research must transition from accessibility to accountability. The Nature Medicine findings serve as a stark reminder that if we do not measure the quality of the intervention, we are not truly providing care. The next phase of maternal health research must prioritize the implementation of “real-time” clinical monitoring systems, ensuring that every birth is supported by a system designed for survival rather than just attendance. For stakeholders looking to modernize their clinical infrastructure or improve patient outcomes through evidence-based governance, engaging with verified healthcare compliance advisors is the first step toward closing the quality gap.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.