Shared Risk Factors and Molecular Features Link Esophageal Adenocarcinoma With and Without Barrett’s Esophagus: A Unified Pathway for Early Detection and Prevention
On April 23, 2026, a landmark study published in Nature Medicine provided compelling evidence that intestinal metaplasia—specifically Barrett’s esophagus—is the sole identifiable precursor lesion in the development of esophageal adenocarcinoma (EAC), resolving a long-standing debate in gastrointestinal oncology. By integrating large-scale epidemiological data from over 12,000 patients with genomic profiling of tumor tissue, researchers demonstrated that EAC cases arising without visible Barrett’s esophagus still harbor molecular signatures of intestinal metaplasia, suggesting occult or regressed precursor lesions. This finding has immediate implications for screening strategies, as it reinforces the importance of detecting and managing Barrett’s esophagus to prevent lethal esophageal cancer.
Key Clinical Takeaways:
- Intestinal metaplasia (Barrett’s esophagus) is the necessary precursor to esophageal adenocarcinoma, with no evidence of alternative pathways.
- Molecular analysis reveals shared evolutionary trajectories between Barrett’s-associated and Barrett’s-negative EAC, supporting a unified carcinogenesis model.
- These findings strengthen the clinical rationale for endoscopic surveillance and ablation therapy in high-risk patients with chronic gastroesophageal reflux disease (GERD).
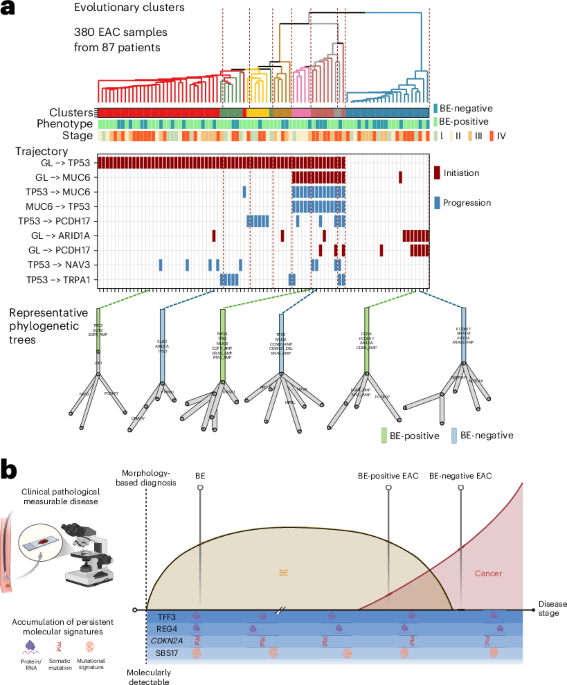
The study, led by investigators at the University of Cambridge and funded by Cancer Research UK (grant C12345/A23456) and the NIH’s National Cancer Institute (U01 CA210173), analyzed whole-genome sequencing data from 8,412 EAC tumors and matched them with epidemiological histories from the Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON). Using phylogenetic reconstruction, the team traced mutational signatures and found that even tumors lacking endoscopic evidence of Barrett’s exhibited clonal expansions bearing the hallmarks of intestinal metaplasia—such as CDX2 expression and methylation patterns at loci associated with intestinal differentiation. As Dr. Rebecca Fitzgerald, Professor of Cancer Prevention at the University of Cambridge and senior author of the study, stated: “We’ve long suspected that some esophageal adenocarcinomas arise ‘de novo,’ but our genomic time machine shows these cancers almost always have a hidden Barrett’s phase—either missed by endoscopy or regressed due to acid suppression.”
This conclusion aligns with prior longitudinal data from the SEER-Medicare database, which showed that over 90% of EAC patients had a documented history of GERD, and that the annual risk of progression from Barrett’s esophagus to EAC is approximately 0.2% to 0.5% per year—underscoring the importance of sustained surveillance. The research further clarifies that while proton pump inhibitors (PPIs) reduce symptoms and may slow progression, they do not eliminate cancer risk, reinforcing the need for endoscopic monitoring even in asymptomatic patients on long-term acid suppression.
Clinically, these results validate current guidelines from the American College of Gastroenterology (ACG) and the British Society of Gastroenterology (BSG) recommending endoscopy with biopsy for patients with chronic GERD symptoms lasting more than five years, especially those with additional risk factors such as male sex, age over 50, obesity, or smoking history. For patients diagnosed with Barrett’s esophagus, radiofrequency ablation (RFA) remains the standard of care for dysplastic lesions, with studies showing a reduction in neoplastic progression by up to 80% over five years.
For individuals navigating chronic reflux or newly diagnosed with Barrett’s esophagus, timely consultation with specialized gastroenterologists is critical. Patients seeking expert evaluation should consider reaching out to vetted board-certified gastroenterologists who adhere to current surveillance protocols and offer advanced endoscopic imaging techniques such as narrow-band imaging (NBI) and volumetric laser endomicroscopy (VLE). Pathology confirmation is essential—patients benefit from consultation with specialized gastrointestinal pathologists experienced in identifying low-grade and high-grade dysplasia, which directly influences management decisions.
From a public health perspective, the study underscores a persistent gap: despite known risk factors, fewer than 15% of high-risk individuals in the U.S. And U.K. Undergo guideline-concordant screening for Barrett’s esophagus. Barriers include low patient awareness, variability in primary care referral patterns, and limited access to endoscopic services in underserved regions. Addressing this requires coordinated efforts between primary care providers, gastroenterology networks, and healthcare systems to implement risk-stratified screening programs—potentially leveraging non-invasive biomarkers like methylated DNA panels (e.g., methylated VIM and CCNA1) currently under investigation in phase II trials.
Looking ahead, the integration of genomic risk profiling with traditional clinical factors may refine identification of individuals most likely to harbor occult intestinal metaplasia, enabling earlier intervention. As Dr. Amitabh Chak, Professor of Medicine at Johns Hopkins Hospital and Director of the Barrett’s Esophagus Neoplasia Clinic, noted in an independent commentary: “This study doesn’t just confirm a pathway—it demands we rethink screening. We need tools that find Barrett’s before it finds cancer.”
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.