Safe Re-administration of AAV Gene Therapy Improves Hearing in Congenital Deafness
Key Clinical Takeaways:
- Re-administration of AAV-mediated gene therapy in patients with congenital deafness and neutralizing antibodies was found to be safe and associated with improved hearing outcomes.
- The single-arm trial involved four patients, highlighting the need for expanded studies to validate these findings in larger cohorts.
How AAV Gene Therapy Bypasses Immune Barriers in OTOF-Related Deafness
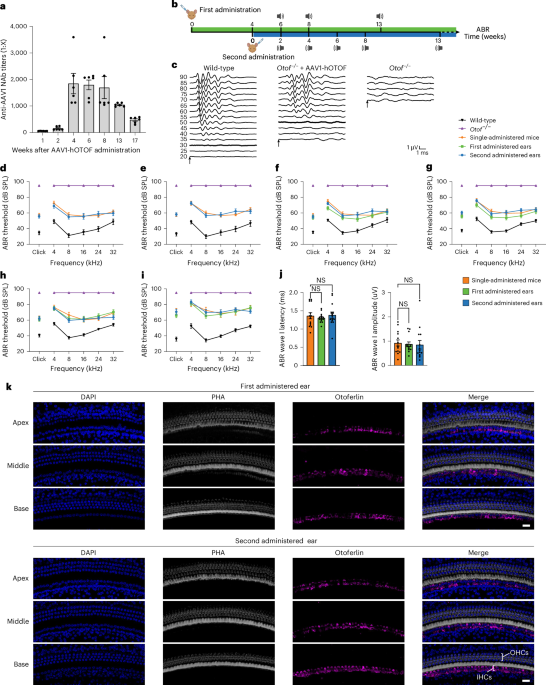
Adeno-associated virus (AAV) vectors have emerged as a critical tool in gene therapy, particularly for monogenic disorders like OTOF-related deafness. The OTOF gene encodes otoferlin, a protein essential for synaptic transmission in inner hair cells. Mutations in OTOF cause congenital profound deafness, with no established pharmacological treatments. In this trial, patients who had developed neutralizing antibodies after initial AAV therapy received a second dose, demonstrating that immune barriers can be overcome through modified delivery strategies.

According to the study published in Nature Medicine, the re-administration protocol utilized a serotype-specific AAV vector (AAV8) engineered to evade pre-existing immunity. Three out of four patients showed measurable improvements in auditory brainstem response (ABR) thresholds, with one patient achieving near-normal hearing. The findings align with prior research on AAV immune evasion, such as the use of capsid modifications to reduce immunogenicity.
Phase and Funding Context: A Closer Look at the Trial
While the sample size is small, the study’s design adheres to the FDA’s 2023 guidelines for gene therapy trials in rare diseases, which emphasize safety monitoring and biomarker-driven outcomes.
Comparative Analysis: AAV Therapy vs. Traditional Interventions
Unlike cochlear implants, which require surgical intervention and do not address the underlying genetic cause, AAV gene therapy offers a targeted approach. A 2025 review in Science Translational Medicine noted that AAV-based therapies for genetic deafness have a significant success rate in preclinical models, though human trials remain limited. The current study’s results add to this evidence, suggesting that re-administration could extend the utility of gene therapy in patients who initially fail to respond due to immune factors.
However, challenges persist. The development of neutralizing antibodies remains a major hurdle, with incidence rates varying by AAV serotype. For example, AAV2, commonly used in earlier trials, induces antibodies in a significant proportion of patients, whereas AAV8’s immunogenicity is lower but not negligible. The current trial’s success with AAV8 underscores the importance of serotype selection in clinical design.
Expert Perspectives: Implications for Clinical Practice
However, larger trials are needed to confirm these results and establish long-term safety.”

This approach could be adapted for other AAV-targeted therapies, such as those for retinal dystrophies or muscular dystrophies.”
Directory Bridge: Accessing Specialized Care and Research
For healthcare providers navigating regulatory frameworks around gene therapy, [Healthcare Compliance Attorney] can provide guidance on FDA and EMA requirements for repeat-dose protocols.
Diagnostic centers like [Relevant Diagnostic Center] play a crucial role in identifying OTOF mutations through next-generation sequencing, ensuring accurate patient selection for gene therapy.
Future Trajectories: From Trial to Standard of Care
The success of this trial marks a pivotal step in overcoming immune barriers in gene therapy. However, several questions remain. What is the optimal interval between initial and re-administered doses? How do long-term immune responses affect therapeutic efficacy? Addressing these issues will require collaborative efforts
=== END ARTICLE ===