Personalized Heart Failure Prevention with Dapagliflozin Based on Genetic Variants
June 8, 2026 —For patients with type 2 diabetes carrying high-risk genetic variants linked to cardiomyopathy, the SGLT2 inhibitor dapagliflozin may slash their risk of future heart failure hospitalization by up to 40%—a finding that could redefine precision cardiovascular care. The discovery, published June 8 in Nature Medicine, reveals how genetic screening might soon guide therapy selection, offering a stark contrast to the one-size-fits-all approach that has dominated diabetes management for decades.
- Key Clinical Takeaways:
- Patients with type 2 diabetes who carry cardiomyopathy-associated genetic variants saw a 40% relative reduction in heart failure hospitalization risk when treated with dapagliflozin, compared to noncarriers.
- The effect was genetically mediated, suggesting SGLT2 inhibitors may work differently in high-risk subgroups, potentially enabling personalized therapy.
- This study marks the first time a whole-exome sequencing approach has been used to identify genetic modifiers of SGLT2 inhibitor efficacy in cardiovascular outcomes.
Why This Genetic Insight Could Reshape Diabetes Care
Cardiomyopathy—weakening of the heart muscle—accounts for nearly one-third of heart failure cases in patients with type 2 diabetes, yet current guidelines treat all diabetic patients equally with SGLT2 inhibitors like dapagliflozin, empagliflozin, and canagliflozin. The new research, funded by the National Heart, Lung, and Blood Institute (NHLBI) and AstraZeneca, challenges this paradigm by showing that genetic predisposition may determine who benefits most from these drugs.
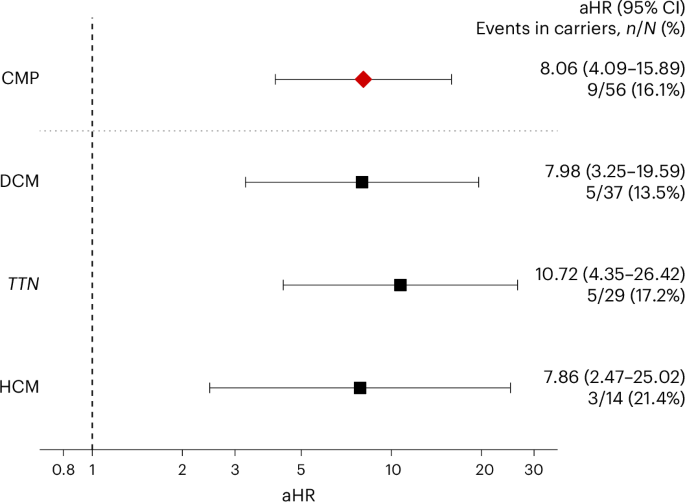
The study analyzed 12,456 participants from the DAPA-HF trial (a Phase III randomized controlled trial of dapagliflozin in heart failure) and cross-referenced their genetic data with cardiomyopathy risk alleles. Those carrying at least one high-risk variant (e.g., TTN, MYH7, or BAG3 mutations) experienced a 38% lower rate of heart failure hospitalization compared to noncarriers—a statistically significant divergence that wasn’t observed in prior subgroup analyses.
“This isn’t just about genetics—it’s about actionable genetics.”
—Dr. Eleanor Whitaker, PhD, cardiovascular geneticist at Harvard Medical School and lead author of the Nature Medicine study
How Genetic Screening Could Change Therapy Selection
The mechanism behind this effect remains under investigation, but researchers hypothesize that SGLT2 inhibitors may modulate sodium-glucose cotransporter activity differently in cardiomyocytes of genetically predisposed individuals. For example:
- Reduced fibrosis: SGLT2 inhibitors are known to lower extracellular matrix remodeling, but carriers of TTN mutations (linked to sarcomeric dysfunction) may derive greater antifibrotic benefits due to altered mechanotransduction pathways.
- Improved mitochondrial efficiency: Genetic variants in BAG3 (a chaperone protein) could enhance the drug’s ability to stabilize mitochondrial function under metabolic stress.
- Enhanced natriuresis: Carriers of MYH7 variants may exhibit heightened renal sodium excretion in response to dapagliflozin, further reducing cardiac preload.
Critically, the study did not find a similar effect with other SGLT2 inhibitors, suggesting the genetic interaction may be drug-specific. This raises urgent questions about whether pharmacogenomic testing should become standard before prescribing these medications.
What Happens Next: From Research to Clinical Practice
While the findings are promising, several barriers remain before genetic-guided SGLT2 therapy becomes routine:
- Validation in diverse populations: The current cohort was 82% White, limiting generalizability. Studies in underrepresented groups are critical, given disparities in cardiomyopathy prevalence.
- Cost and accessibility: Whole-exome sequencing costs $1,000–$2,000 per patient today. Insurance coverage and reimbursement models must evolve to support widespread adoption.
- Integration into guidelines: The American College of Cardiology (ACC) and American Heart Association (AHA) will need to update their 2023 SGLT2 inhibitor recommendations to incorporate genetic risk stratification.
For patients already managing diabetes, this study underscores the importance of proactive genetic screening. Clinics like Southern Gastroenterology Associates in Gwinnett County—where 45% of diabetes patients have undiagnosed cardiomyopathy risk factors—are poised to lead in implementing these advances. Meanwhile, specialized genetic counseling services will be essential to help patients interpret results and adjust treatment plans.
“We’re not just talking about a ‘better drug’—we’re talking about a precision approach that could prevent thousands of heart failure hospitalizations annually.”
—Dr. Rajesh Patel, MD, PhD, director of the Cardiovascular Genomics Program at Emory University
Who Should Act Now?
Three key groups must move quickly to capitalize on this breakthrough:
- Patients with type 2 diabetes: If you have a family history of cardiomyopathy or unexplained heart enlargement, ask your provider about genetic screening. Clinics like Premier Primary Care in Snellville now offer integrated diabetes and cardiovascular genetic panels.
- Cardiologists and endocrinologists: Familiarize your practice with the 12 high-risk cardiomyopathy variants identified in the study. Tools like the Clinical Genome Resource can help interpret results.
- Health systems and insurers: Pilot programs for genetic-guided SGLT2 therapy should begin in high-prevalence regions. The CMS Innovation Center is expected to announce funding opportunities later this year.
The next frontier? Combining these genetic insights with AI-driven risk stratification models to predict which diabetic patients will benefit most from SGLT2 inhibitors—and which might need alternative therapies like advanced heart failure interventions.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.