NHS Lung Cancer Screening: Early Results & Lessons from England’s National Program
The NHS England Lung Cancer Screening Programme, formerly known as the Targeted Lung Health Check (TLHC) Programme, has rapidly scaled up to offer screening to those at highest risk of developing the disease, with early data suggesting a positive impact on the stage at which lung cancer is diagnosed.
Launched nationally on February 1, 2025, following a recommendation from the UK National Screening Committee, the program aims to detect lung cancer earlier, when treatment is more likely to be successful. As of early 2026, almost one-third of England’s estimated eligible population has received invitations to participate, demonstrating the feasibility of large-scale implementation.
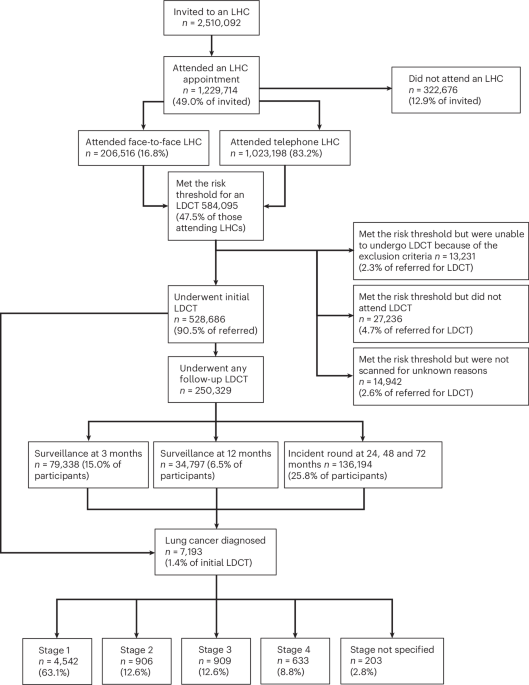
The program targets individuals aged 55 to 74 with a history of smoking. Participants undergo an initial lung health check, and those deemed high-risk are offered a low-dose computed tomography (CT) scan. Initial results indicate that 1.4% of participants have been diagnosed with lung cancer, with 76% of those diagnoses occurring at stages 1 or 2 – an earlier stage than typically seen in patients diagnosed outside of the screening program. Over 75% of cancers detected through screening have been at stages 1 or 2, compared to less than 30% detected through standard routes.
This shift towards earlier-stage diagnoses is already reflected in national lung cancer registry data, which shows an increase in early-stage diagnoses coinciding with the rollout of the screening program. Notably, this trend has not been observed in other cancer types in England, suggesting a direct impact from the screening initiative. The latest UK National Lung Cancer Audit reports increases in lung cancer incidence, stage 1 rates and surgical resection rates.
The program’s delivery model has proven adaptable. The majority (83.2%) of lung health checks are now conducted by telephone, a change implemented in response to the COVID-19 pandemic and found to be both feasible and efficient. While adherence to a standard protocol and quality assurance standards is mandated, the program allows for innovation, with proposed changes reviewed by a national operations team and clinical advisory committee.
Uptake of the screening offer currently stands at 49.0%, lower than other national screening programs. Initial targeting focused on areas with high socioeconomic deprivation, where uptake rates are generally lower. Analysis of early data confirms that individuals from the most deprived socioeconomic groups and non-white communities are less likely to respond to invitations. However, uptake is improving, with recent data indicating rates exceeding 60%, a figure comparable to international experience in lung cancer screening.
Despite improvements, concerns remain about the significant proportion of eligible individuals who do not participate. Given that socioeconomic disadvantage is linked to both lower participation and increased lung cancer risk, a disproportionate number of those who could benefit from screening are being missed.
In January 2025, the program underwent a name change from the Targeted Lung Health Check to the NHS Lung Cancer Screening Programme, a decision informed by behavioral science research indicating that “lung cancer screening” was less ambiguous and more readily understood by the public. However, participants continued to prefer the term “lung health check” when referring to the initial risk assessment.
The program utilizes multivariable risk models to determine eligibility, a strategy chosen based on evidence demonstrating their efficiency in identifying individuals at risk of lung cancer. While the cancer detection rate of 1.4% is slightly lower than observed in the UK Lung Screening trial, it remains comparable to, or exceeds, rates reported in large randomized trials and is higher than rates currently seen in the USA.
Data also reveals some demographic disparities in participation. Fewer women attend lung health checks overall and are less likely to be assessed as high risk. Lower uptake was also observed among individuals from more deprived backgrounds, although these participants were more likely to be identified as high risk and to have screen-detected cancer, likely due to higher smoking rates. Significant differences in uptake were also noted based on ethnicity, with individuals from white ethnic backgrounds being markedly more likely to attend than those from other ethnicities (62.5% versus 18.8%). These disparities are being closely monitored and will inform future program design to address inequities.
The program has also focused on managing incidental findings discovered during screening, with a protocol in place to guide appropriate follow-up. The protocol prioritizes action on findings where there is a clear potential for benefit, such as prompting reminders for primary prevention measures for participants with moderate or severe coronary artery calcification. Nationally standardized pathways for managing incidental findings have been implemented to address concerns about overdiagnosis and workload pressures.
The expansion of the screening program has placed demands on existing healthcare services, requiring increased surgical and oncology capacity. New sites are learning from earlier adopters about the need for service expansion and workforce development. The program utilizes both locally outsourced capacity for call provision and CT scanning, including mobile units and radiology reporting.
NHS England is currently developing 14 effectiveness standards, currently in consultation, designed to provide a basis for performance management and quality assurance of outcomes. A bespoke, end-to-end participant-level information technology system is expected to be implemented by mid-2026.