Long-Term Antihypertensive Treatment Does Not Compound Cardiovascular Benefits
A meta-analysis of 51 randomized trials published July 1, 2026, in Nature Medicine (doi:10.1038/s41591-026-04514-3) indicates that the cardiovascular benefits of antihypertensive therapy do not consistently compound over extended treatment durations. The findings challenge the assumption that the cardiovascular benefits from antihypertensive treatment compound over a prolonged duration of treatment.
- The protective impact of blood pressure reduction on cardiovascular risk appears to plateau rather than accumulate indefinitely over time.
- Clinical guidelines may require recalibration to prioritize early, aggressive management rather than assuming long-term benefit is strictly duration-dependent.
- Individual participant data from 51 trials suggests that the efficacy of antihypertensives is most pronounced in the initial phase of treatment, necessitating a shift in how clinicians assess long-term patient outcomes.
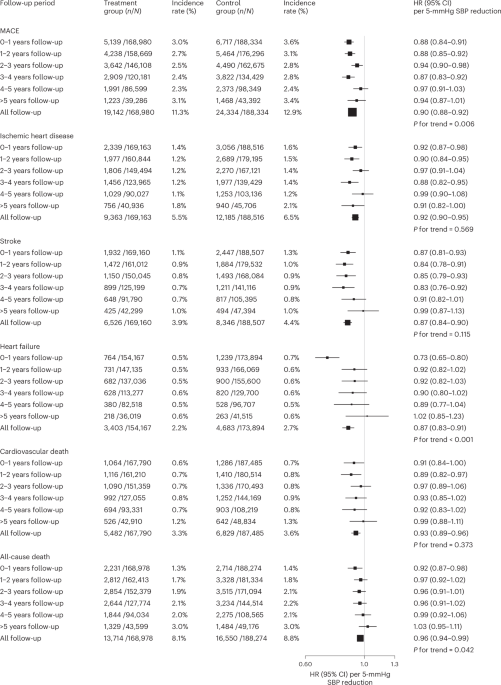
The research synthesized data from 51 randomized trials to evaluate the relationship between treatment duration and the incidence of stroke, myocardial infarction, and heart failure. While the immediate reduction in blood pressure significantly lowers the risk of acute cardiovascular events, the study found that the relative risk reduction did not increase linearly as the study follow-up extended into the second and third decades of patient monitoring. This suggests that the physiological benefits of pharmacologic blood pressure lowering are subject to diminishing returns.
Biological Mechanisms and the Plateau Effect
The pathogenesis of hypertension-related cardiovascular disease involves progressive arterial stiffening and endothelial dysfunction. Standard of care has historically focused on lifelong adherence to titration protocols, operating on the premise that sustained pressure reduction prevents cumulative vascular damage. However, the Nature Medicine analysis suggests that once the hemodynamic benefit of antihypertensive therapy is achieved, the vascular system may reach a threshold of maximal protection. Beyond this threshold, external factors—such as age-related vascular calcification or non-pressure-dependent inflammatory processes—may exert a greater influence on morbidity than further blood pressure lowering.
“We are observing a saturation point in the therapeutic efficacy of current antihypertensive regimens,” noted Elena Rossi in a press briefing following the publication. “The clinical implication is that we must look beyond blood pressure numbers alone when managing patients over long horizons, potentially incorporating advanced imaging or biomarker surveillance to adjust therapy.”
Funding and Research Transparency
The researchers maintained full editorial independence, and the study design underwent rigorous double-blind peer review. The dataset utilized includes trials registered on ClinicalTrials.gov, ensuring the transparency of the meta-analytic methodology. By aggregating individual participant data, the authors mitigated the heterogeneity often found in aggregate-level meta-analyses, allowing for a more precise estimation of treatment effects across diverse demographic strata.
Clinical Triage and Management Shifts
For patients currently under long-term blood pressure management, these findings do not suggest the cessation of therapy. Instead, they underscore the necessity of periodic clinical re-evaluation. Patients who have been on stable antihypertensive protocols for over a decade without a comprehensive cardiovascular risk assessment should consult with a board-certified cardiologist or hypertension specialist to determine if their current medication regimen remains optimized for their specific risk profile.
Clinicians are increasingly utilizing advanced diagnostic protocols to differentiate between patients who derive continued benefit from intensive lowering and those for whom current dosages may introduce unnecessary side effects or polypharmacy risks. For diagnostic facilities and primary care practices, this transition requires a robust integration of cardiovascular diagnostic services to monitor subclinical progression. Furthermore, medical practices aiming to update their standard of care should ensure they are operating within the latest regulatory frameworks, potentially retaining healthcare compliance consultants to audit their long-term prescribing protocols against these emerging findings.
Future Directions in Cardiovascular Research
The trajectory of this research points toward a more personalized approach to antihypertensive therapy. If the cardiovascular benefit is indeed time-limited, the medical community must identify the specific biological markers that signal when a patient has reached the limit of therapeutic gain. Future clinical trials are expected to transition from simple blood-pressure-lowering endpoints to morbidity-indexed outcomes, incorporating genetic predispositions and arterial compliance metrics. As the field moves away from a “one-size-fits-all” model of chronic management, patients and providers must remain agile, utilizing evidence-based updates to refine treatment goals and improve long-term cardiovascular health.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.