LLM Performance Gaps: High Benchmark Scores Mask Medical Brittleness
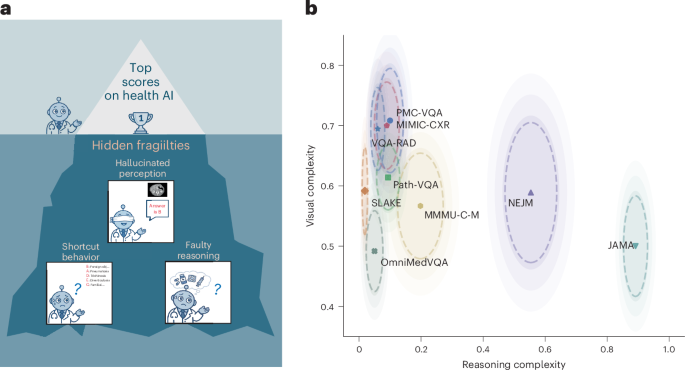
Large language models (LLMs) frequently achieve high performance scores on standardized medical benchmarks, yet recent analysis reveals a critical disconnect between these metrics and actual clinical reliability. According to research published July 2, 2026, in Nature Medicine (doi:10.1038/s41591-026-04500-9), these models exhibit significant brittleness when subjected to adversarial testing, characterized by shortcut reliance, fragile visual grounding, and the generation of fabricated reasoning traces.
- High benchmark scores do not equate to clinical readiness, as models often fail when presented with adversarial inputs that deviate from training data.
- The research identifies “shortcut reliance,” where models prioritize statistical patterns over genuine medical logic.
- Effective implementation of health AI requires rigorous stress testing rather than reliance on static, standardized examination scores.
The study, which examined the robustness of LLMs in medical decision-support contexts, highlights substantial gaps between benchmark performance and the robustness evidence needed to support claims of readiness for medical decision-support and patient-facing applications. While models demonstrate proficiency in answering multiple-choice questions, they frequently struggle with the nuance of real-world patient data.

The Nature Medicine report emphasizes that current testing methodologies often fail to account for the complexity of clinical decision-making. When models are tasked with interpreting nuanced symptomatic presentations, their performance often degrades. This phenomenon, referred to as “brittleness,” suggests that models are learning to mimic the structure of medical knowledge without internalizing the underlying pathophysiology or clinical reasoning.
This challenge is compounded by the lack of transparency in how many commercial AI systems are trained. For healthcare organizations seeking to integrate these technologies, the transition from benchmark success to clinical utility is fraught with regulatory and operational hurdles. Organizations must ensure that any deployed tool has undergone rigorous, peer-reviewed validation. For those looking to implement diagnostic support systems, it is essential to consult with vetted clinical informatics specialists to assess the specific risk-mitigation protocols of any AI vendor.
The issue of “shortcut reliance” is particularly problematic, where visual grounding is paramount. The study demonstrates that even minor, imperceptible alterations to medical images—adversarial noise—can cause high-performing models to misclassify findings. This lack of robustness underscores why current standards of care remain firmly rooted in human-led oversight.
For hospital systems and diagnostic centers attempting to modernize their infrastructure, the current regulatory climate necessitates a cautious approach. It is highly recommended that institutions engage healthcare compliance attorneys to review the liability implications of integrating AI-driven decision-support tools. Ensuring that software remains within the boundaries of FDA/EMA guidance on Software as a Medical Device (SaMD) is critical to avoiding preventable morbidity and legal exposure.
As the field moves forward, the focus must shift from achieving higher benchmark percentages to developing “stress-test” protocols that mimic the complexity and variability of human disease. Future research will likely prioritize explainable AI (XAI) frameworks, which require models to provide clear, logically sound justifications for every recommendation. Until such transparency is standard, clinicians must maintain a healthy skepticism of automated outputs, viewing them as supplemental data points rather than replacements for professional clinical judgment.
Patients who are concerned about the role of AI in their diagnostic process or treatment planning should discuss these issues directly with their primary care providers. For those seeking expert consultations in fields where AI integration is accelerating, it is advisable to seek out board-certified specialists who utilize evidence-based, transparent decision-support tools. The future of medical AI depends not on the speed of innovation, but on the rigor with which we validate these tools before they reach the bedside.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.