Isatuximab Improves MRD Negativity in Newly Diagnosed Multiple Myeloma: Phase 3 IsKia Trial
The pursuit of a “deep response” in multiple myeloma has shifted from simple clinical remission to the rigorous standard of measurable residual disease (MRD) negativity. Achieving this state—where no cancer cells are detectable even with highly sensitive technology—is increasingly viewed as the gold standard for prolonging progression-free survival in transplant-eligible patients.
Key Clinical Takeaways:
- The Isa-KRd quadruplet therapy significantly increased MRD negativity rates compared to the KRd triplet, reaching 77% versus 67% at the 10⁻⁵ sensitivity level.
- Deep responses were achieved faster during the induction phase and remained more durable over a one-year period.
- The addition of isatuximab did not significantly increase the rate of Grade 3–4 non-hematologic adverse events or treatment discontinuations.
For years, the clinical community has debated the optimal combination of agents for patients with newly diagnosed multiple myeloma (NDMM) who are eligible for autologous stem cell transplantation (ASCT). While triplet therapies—combining a proteasome inhibitor, an immunomodulatory drug, and dexamethasone—have long been the standard of care, the integration of CD38-targeting monoclonal antibodies into a quadruplet regimen represents a strategic attempt to close the gap in treatment efficacy. The primary clinical hurdle is not merely achieving a response, but ensuring that the response is deep enough to prevent early relapse, a goal measured by next-generation sequencing (NGS).
The IsKia Trial: Architecture and Patient Cohort
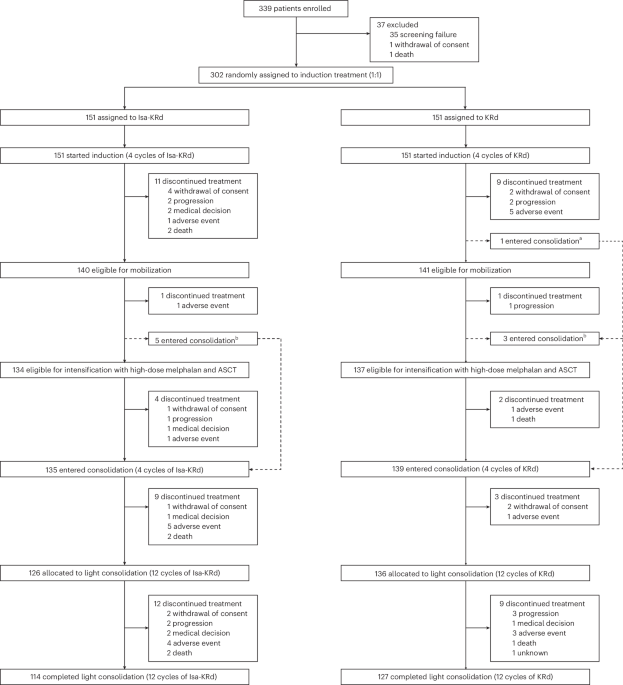
The phase 3 EMN24 IsKia trial, as detailed in a study published in Nature Medicine, randomized 302 transplant-eligible patients aged 70 years or younger. The study was designed to compare the efficacy and safety of a quadruplet regimen—isatuximab, carfilzomib, lenalidomide, and dexamethasone (Isa-KRd)—against the triplet standard of carfilzomib, lenalidomide, and dexamethasone (KRd). This research was conducted through the European Myeloma Network to establish whether the addition of a CD38 antibody could fundamentally alter the depth of the response.

The treatment protocol was rigorous, structured across four distinct phases to maximize the eradication of malignant plasma cells. Patients first underwent four cycles of induction therapy, followed by ASCT. Post-transplant, they received four cycles of consolidation therapy, which was then followed by 12 cycles of “light consolidation.” This sequential approach ensures that the bone marrow is primed for transplantation and that any remaining clones are targeted during the consolidation phase. For patients navigating these complex multi-phase protocols, coordinating care between board-certified hematologists and transplant coordinators is essential to maintain the strict timing required for optimal outcomes.
Analyzing the Depth of Response: MRD Negativity
The primary endpoint of the IsKia trial was the rate of MRD negativity with a sensitivity of 10⁻⁵ or better, measured via NGS after the consolidation phase. The results indicate a statistically significant advantage for the Isa-KRd arm. At the 10⁻⁵ threshold, 77% of patients in the Isa-KRd group achieved MRD negativity compared to 67% in the KRd group. The divergence became even more pronounced at the more stringent 10⁻⁶ sensitivity level, where the Isa-KRd arm reached 68% negativity versus only 48% for the KRd arm.
These findings suggest that the addition of isatuximab doesn’t just improve the likelihood of a response, but increases the probability of a “deep” response. The speed of this response is equally critical; post-induction MRD negativity at the 10⁻⁵ level was 46% for Isa-KRd compared to 27% for KRd. This rapid clearance of detectable disease prior to transplantation may potentially reduce the risk of early relapse. As these measurements rely on high-sensitivity NGS, patients require access to specialized diagnostic centers capable of performing 10⁻⁶ sensitivity testing to accurately monitor their disease status.
| Metric (MRD Negativity) | Isa-KRd (Quadruplet) | KRd (Triplet) | Odds Ratio (OR) / P-value |
|---|---|---|---|
| Post-Consolidation (10⁻⁵) | 77% | 67% | OR 1.67, P = 0.049 |
| Post-Consolidation (10⁻⁶) | 68% | 48% | OR 2.36, P = 0.0004 |
| Post-Induction (10⁻⁵) | 46% | 27% | OR 2.32, P = 0.0007 |
| Post-Induction (10⁻⁶) | 28% | 14% | OR 2.44, P = 0.0029 |
| 1-Year Sustained (10⁻⁶) | 52% | 38% | OR 1.82, P = 0.012 |
Safety Profiles and Clinical Tolerability
A recurring concern when escalating from triplet to quadruplet therapy is the potential for increased morbidity and treatment-related toxicity. In the IsKia trial, though, the safety profile remained manageable. The data indicate that Grade 3–4 non-hematologic adverse events were similar across both the Isa-KRd and KRd arms. There were no significant differences in the rates of treatment discontinuations or deaths resulting from adverse events.
This balance of increased efficacy without a corresponding spike in severe toxicity is a critical finding. It suggests that the pathogenesis of the disease can be more aggressively targeted without compromising the patient’s ability to complete the full course of induction and consolidation. However, the long-term impact on progression-free survival (PFS) remains to be fully determined, as the data at the time of the ClinicalTrials.gov (NCT04483739) report were still immature.
The Future of Quadruplet Induction
The IsKia trial provides strong evidence that adding isatuximab to the KRd backbone enhances the depth and durability of the response in transplant-eligible NDMM patients. By achieving higher rates of 10⁻⁶ MRD negativity—sustained in 52% of patients at one year compared to 38% in the control group—the Isa-KRd regimen sets a new benchmark for what constitutes a successful induction and consolidation phase.
As the medical community moves toward MRD-driven treatment decisions, the ability to identify patients who fail to achieve these deep responses will be paramount. This will likely lead to more personalized “triage” strategies, where therapy is intensified for those who remain MRD-positive after consolidation. For healthcare providers and clinics, incorporating these high-sensitivity NGS protocols is no longer optional but a necessity for precision oncology. Patients seeking to integrate these emerging quadruplet therapies into their care plan should consult with vetted oncology specialists to determine if their specific clinical profile aligns with the eligibility criteria established in the EMN24 trials.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.