Everolimus Shows Promise in Biomarker-Driven Trial for Newly Diagnosed Diffuse Intrinsic Pontine Glioma Despite Unmet Primary Endpoint
On April 24, 2026, Nature Medicine published results from the randomized Phase 2 BIOMEDE trial, a biomarker-driven study evaluating the addition of targeted therapies—erlotinib, everolimus, or dasatinib—to standard radiotherapy in children newly diagnosed with diffuse intrinsic pontine glioma (DIPG). While the primary endpoint of overall survival was not met across any treatment arm, the trial identified molecular and clinical features associated with long-term survival and positioned everolimus as a promising candidate for further investigation in this universally lethal pediatric brain tumor.
Key Clinical Takeaways:
- Adding erlotinib, everolimus, or dasatinib to radiotherapy did not significantly improve overall survival in children with newly diagnosed DIPG in the BIOMEDE trial.
- Biomarker analysis revealed that tumors with H3K27M mutation and low PDGFRA expression were associated with longer survival, offering potential stratification tools for future trials.
- Everolimus showed a favorable signal in exploratory analyses, warranting further study as a potential component of multimodal therapy for DIPG.
Diffuse intrinsic pontine glioma remains one of the most devastating diagnoses in pediatric oncology, accounting for approximately 10-15% of all childhood brain tumors but causing a disproportionate share of mortality due to its infiltrative growth within the brainstem, which precludes surgical resection. Despite decades of research, the standard of care has remained focal radiotherapy—typically 54 Gy in 30 fractions—with no chemotherapy or targeted agent demonstrating a consistent survival benefit in Phase III trials. The median overall survival remains 9 to 12 months from diagnosis, and fewer than 10% of patients survive two years. The BIOMEDE trial, funded by the European Union’s Horizon 2020 program (grant agreement No. 634579) and coordinated by the French Society for Pediatric Oncology (SFCE), sought to disrupt this stagnation by integrating molecular profiling into treatment assignment.
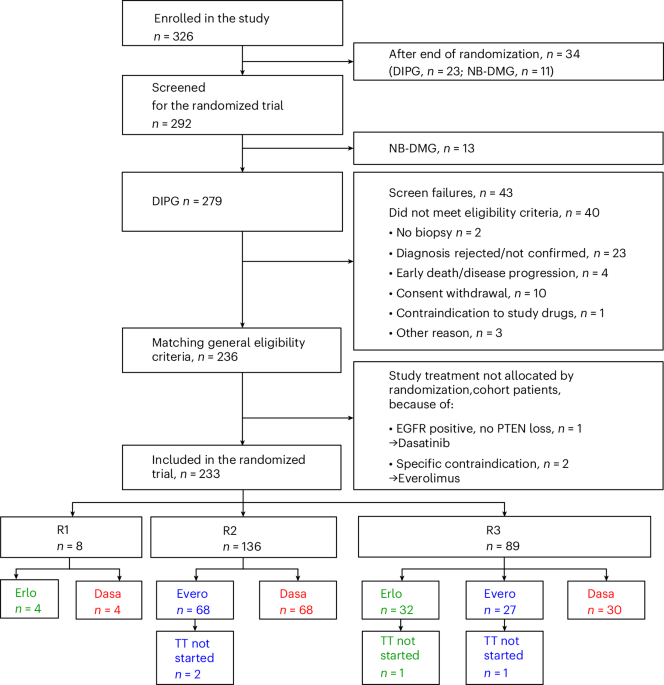
Eligible patients—those aged 1 to 21 years with MRI-confirmed DIPG and no prior treatment—were stratified at diagnosis based on tumor biopsy or cerebrospinal fluid analysis for actionable alterations in the PDGFRA, mTOR, or EGFR pathways. Patients with PDGFRA amplification or mutation received erlotinib (an EGFR/PDGFRA inhibitor), those with mTOR pathway activation received everolimus (an mTORC1 inhibitor), and those with EGFR alterations received dasatinib (a Src/Bcr-Abl inhibitor), all administered concurrently with radiotherapy. The control arm received radiotherapy alone. The primary endpoint was overall survival at 12 months. Secondary endpoints included progression-free survival, safety, and correlative biomarker analysis.
According to the study published in Nature Medicine, 84 patients were enrolled across 27 centers in Europe and Australia between 2016 and 2021. The intention-to-treat analysis showed no statistically significant difference in overall survival between any experimental arm and radiotherapy alone (hazard ratio [HR] for everolimus vs. Radiotherapy: 0.89, 95% CI 0.58–1.37. p=0.60). Similarly, erlotinib (HR 1.02, 95% CI 0.66–1.58) and dasatinib (HR 0.95, 95% CI 0.60–1.50) failed to demonstrate a survival advantage. However, exploratory biomarker analysis revealed that patients whose tumors harbored the H3K27M mutation—a hallmark of >80% of DIPGs—combined with low PDGFRA expression had a median overall survival of 16.7 months, compared to 10.2 months in those with high PDGFRA expression (p=0.03). This suggests that PDGFRA signaling may confer a more aggressive phenotype even within the molecularly defined H3K27M-mutant cohort.
“While the targeted agents did not move the needle on survival as monotherapy companions to radiotherapy, the BIOMEDE trial succeeded in proving that molecularly guided trials are feasible in DIPG. The signal we saw with everolimus, particularly in patients with low PDGFRA expression, suggests that mTOR inhibition may have a role in a subset of tumors where this pathway is genuinely addictive—and that we necessitate smarter biomarkers to identify them.”
The safety profile of the added agents was manageable, with no unexpected toxicities. Grade 3 or 4 adverse events occurred in 32% of patients receiving everolimus (primarily stomatitis and hyperglycemia), 28% in the erlotinib arm (rash and diarrhea), and 25% in the dasatinib arm (fatigue and pleural effusions)—rates consistent with known profiles of these agents in other malignancies. Treatment-related discontinuation occurred in fewer than 10% of patients across all arms, supporting the feasibility of combining these agents with radiotherapy in this fragile population.
Everolimus emerged as the most promising candidate for further study, not only due to its trend toward improved survival but too given that of its mechanistic rationale: the mTOR pathway is frequently activated in DIPG downstream of PDGFRA signaling and may contribute to radiation resistance and tumorigenic persistence. Preclinical models have shown that mTOR inhibition can potentiate the effects of radiotherapy by reducing DNA repair capacity and promoting autophagy-mediated cell death. These findings align with earlier work from the Children’s Oncology Group (COG) ACNS0921 trial, which tested temsirolimus (another mTOR inhibitor) with radiotherapy in recurrent high-grade glioma, though without survival benefit—highlighting the importance of timing, patient selection, and biomarker enrichment in future designs.
For families navigating a DIPG diagnosis, access to specialized neuro-oncologic care and clinical trial expertise is paramount. Institutions with active molecular tumor boards and experience in pediatric central nervous system trials offer the best opportunity for enrollment in innovative studies like BIOMEDE or its successors. It is strongly recommended to consult with vetted board-certified pediatric neuro-oncologists who can guide biopsy decisions, molecular testing, and trial eligibility assessment. Advanced diagnostic centers equipped for cerebrospinal fluid analysis and intraoperative MRI-guided biopsy—such as those listed under pediatric neurosurgery centers—play a critical role in enabling biomarker-driven approaches. Finally, given the complex ethical and consent challenges inherent in pediatric oncology trials, families may benefit from consulting healthcare compliance attorneys with expertise in research ethics and informed consent to ensure that participation aligns with both medical goals and family values.
As the field moves forward, the BIOMEDE trial underscores a critical lesson: in molecularly heterogeneous diseases like DIPG, blanket application of targeted agents based on pathway activation alone is insufficient. Future trials must integrate dynamic biomarkers—such as longitudinal CSF genotyping or radiomic features—to identify not just who has an alteration, but who is truly dependent on it for tumor survival. The signal with everolimus invites cautious optimism, particularly if tested in biomarker-enriched cohorts or in combination with agents that target parallel resistance mechanisms, such as HDAC inhibitors or immunotherapy modulators. Until then, radiotherapy remains the foundation of care, but trials like BIOMEDE ensure that every incremental insight is rigorously pursued—not as a promise of cure, but as a step toward transforming DIPG from a universally fatal diagnosis into a condition where long-term survival becomes a tangible, if distant, possibility.
“The real victory of BIOMEDE isn’t in the survival curves—it’s in proving People can do science in this disease. We collected biopsies, we assigned therapy based on molecular logic, we followed patients rigorously, and we learned. That infrastructure is now in place, and it will serve the next generation of trials far better than any single drug ever could.”
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.