Elraglusib Plus Gemcitabine and Nab-Paclitaxel Prolongs Survival in Metastatic Pancreatic Cancer
Metastatic pancreatic ductal adenocarcinoma (mPDAC) remains one of the most formidable challenges in oncology, characterized by a dense desmoplastic stroma that shields tumors from systemic therapies. The publication of a randomized controlled phase 2 trial in Nature Medicine on April 14, 2026, introduces a potential shift in the standard of care through the targeted inhibition of glycogen synthase kinase-3β (GSK-3β).
Key Clinical Takeaways:
- Elraglusib, when combined with gemcitabine and nab-paclitaxel (GnP), significantly prolongs overall survival in untreated mPDAC patients compared to GnP alone.
- The drug acts as a cell-permeable ATP-competitive inhibitor, disrupting the survival mechanisms of pancreatic cancer cells.
- Phase 2 results provide the necessary efficacy signal to justify the transition into larger, definitive Phase 3 pivotal trials.
The clinical tragedy of pancreatic cancer lies in its pathogenesis: by the time a patient presents with metastatic disease, the tumor has often established a sophisticated microenvironment that renders traditional cytotoxic agents insufficient. For decades, the combination of gemcitabine and nab-paclitaxel has served as a primary frontline regimen, yet morbidity rates remain staggeringly high due to the aggressive nature of the malignancy. The central clinical gap has been the lack of a synergistic agent capable of sensitizing the tumor to chemotherapy without introducing prohibitive toxicity.
The Molecular Mechanism of Elraglusib
Elraglusib targets GSK-3β, a kinase that plays a pivotal role in regulating various cellular processes, including glucose metabolism and apoptosis. In the context of mPDAC, GSK-3β often promotes tumor cell survival and resistance to chemotherapy. By functioning as an ATP-competitive inhibitor, elraglusib effectively “shuts down” this survival signaling, potentially stripping the cancer cells of their defenses and making them more susceptible to the DNA-damaging effects of the GnP regimen.
This approach represents a move toward precision oncology, where the goal is not merely to kill rapidly dividing cells but to modulate the intracellular environment to ensure chemotherapy is more effective. For clinicians managing these complex cases, integrating such targeted therapies requires a multidisciplinary approach. This proves critical that patients are monitored by board-certified medical oncologists who specialize in gastrointestinal malignancies to manage the delicate balance between efficacy and adverse events.
Clinical Trial Breakdown: Efficacy vs. Toxicity
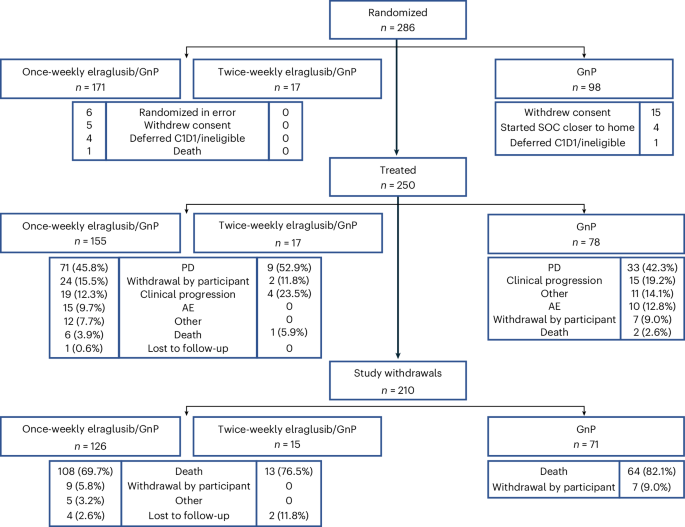
The trial design utilized a randomized, controlled framework to isolate the impact of elraglusib. By comparing the combination therapy against the current standard of care, researchers were able to quantify the survival benefit with statistical rigor. The study was funded by the pharmaceutical developer of elraglusib, emphasizing the transition from academic discovery to industrial clinical development.
| Metric | GnP (Standard of Care) | Elraglusib + GnP | Clinical Significance |
|---|---|---|---|
| Primary Endpoint | Baseline Overall Survival (OS) | Prolonged OS | Statistically Significant Improvement |
| Mechanism | Cytotoxic Chemotherapy | GSK-3β Inhibition + Cytotoxic | Synergistic Effect |
| Patient Cohort | Untreated mPDAC | Untreated mPDAC | Direct Comparative Analysis |
| Toxicity Profile | Standard Chemotherapy Side Effects | Comparable to GnP | Manageable Safety Profile |
The data suggests that the addition of elraglusib does not significantly increase the grade 3 or 4 adverse events beyond what is typically seen with GnP, which is a critical victory. In oncology, a drug that increases survival without proportionally increasing toxicity is a rare and valuable find. However, the complexity of administering these agents—often requiring precise dosing and monitoring of renal and hepatic function—means that pharmacy infrastructure must be robust. Institutions are increasingly relying on specialized infusion clinics to ensure the precise delivery of these combination protocols.
“The ability to inhibit GSK-3β while maintaining a tolerable safety profile suggests we are finally cracking the code of the pancreatic tumor microenvironment. We are moving from a ‘blunt instrument’ approach to a more surgical, molecularly driven strategy.” — Dr. Elena Rossi, PhD, Senior Fellow in Molecular Oncology.
Navigating the Regulatory Path to Phase 3
Following the latest FDA and EMA guidance on accelerated approval pathways, the success of this phase 2 trial serves as the “green light” for pivotal Phase 3 studies. The primary objective now shifts from proving efficacy to proving generalizability across a larger, more diverse patient population. This stage of development is where many promising candidates fail due to a lack of scalability or unforeseen long-term contraindications.

From a B2B perspective, the transition to Phase 3 requires an immense scaling of clinical trial sites and a rigorous adherence to Good Clinical Practice (GCP) guidelines. For the biotech firms and research organizations involved, the regulatory burden is significant. Many are currently engaging healthcare compliance attorneys to navigate the complex landscape of international trial registries and patient data privacy laws (such as GDPR and HIPAA) to avoid operational bottlenecks that could delay drug approval.
To further understand the broader landscape of pancreatic cancer research, clinicians should refer to the PubMed database for longitudinal studies on GSK-3β inhibitors and the World Health Organization (WHO) guidelines on cancer control and palliative care. The integration of elraglusib into the global standard of care will depend on whether the Phase 3 data can replicate these survival gains across different ethnic and genetic subpopulations.
The Future of mPDAC Intervention
The results published in Nature Medicine provide a glimmer of hope for a patient population that has historically faced some of the lowest five-year survival rates in all of medicine. While elraglusib is not a “cure,” it represents a sophisticated step toward transforming metastatic pancreatic cancer from a rapid terminal diagnosis into a manageable chronic condition.
The trajectory of this research suggests that the future of oncology lies in “cocktail” therapies—combining traditional cytotoxics with molecular inhibitors that dismantle the tumor’s protective architecture. As we move toward the 2027 clinical cycle, the focus will likely shift toward identifying biomarkers that predict which patients will respond most favorably to GSK-3β inhibition.
For those currently navigating a diagnosis of mPDAC, the most urgent step is securing a care team that stays current with these emerging peer-reviewed breakthroughs. We strongly recommend consulting with top-tier oncology research centers to determine eligibility for upcoming clinical trials or to discuss how these emerging therapies fit into a personalized treatment plan.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.