Breakthroughs in Cancer Treatment: αKG-Driven DNA Repair & Overcoming Chemotherapy Resistance
A breakthrough in cancer biology has just reshaped how we understand chemotherapy resistance—and the metabolic vulnerabilities hidden inside every cell. Researchers at the Wistar Institute and Temple University have pinpointed a previously overlooked biochemical pathway: α-ketoglutarate (αKG), a metabolic byproduct of the Krebs cycle, directly fuels carnitine synthesis, which in turn enhances DNA repair through histone acetylation. The discovery doesn’t just explain why some ovarian cancer cells shrug off platinum-based therapies—it offers a precision-targeted workaround. But the clinical implications stretch far beyond oncology, touching epigenetic therapy, mitochondrial dysfunction, and even aging. For patients battling treatment-resistant cancers, this could mean the difference between a failed regimen and a tailored metabolic strike.
Key Clinical Takeaways:
- Metabolic bypass discovered: αKG-mediated carnitine synthesis boosts DNA repair via histone acetylation, creating a vulnerability in chemotherapy-resistant cancer cells.
- Ovarian cancer focus: The study identifies a specific metabolic target that could reverse platinum resistance, with Phase I/II trials underway at major cancer centers.
- Broader applications: The pathway may also impact epigenetic therapies, mitochondrial disorders, and even age-related decline in DNA repair efficiency.
The Chemotherapy Resistance Paradox: Why Some Cancers Outsmart Drugs
Platinum-based chemotherapy—cisplatin, carboplatin—has been the cornerstone of ovarian cancer treatment for decades. Yet resistance develops in up to 80% of patients within two years, leaving oncologists with few options (American Cancer Society, 2024). The conventional explanation? Mutations in DNA repair genes like BRCA1/2 or overexpression of efflux pumps. But the Wistar-Temple study, published in Nature and funded by the National Cancer Institute (NCI), reveals a deeper, metabolic flaw: resistant cells aren’t just dodging the drug’s cytotoxic effects—they’re actively repairing the damage faster than healthy cells can.
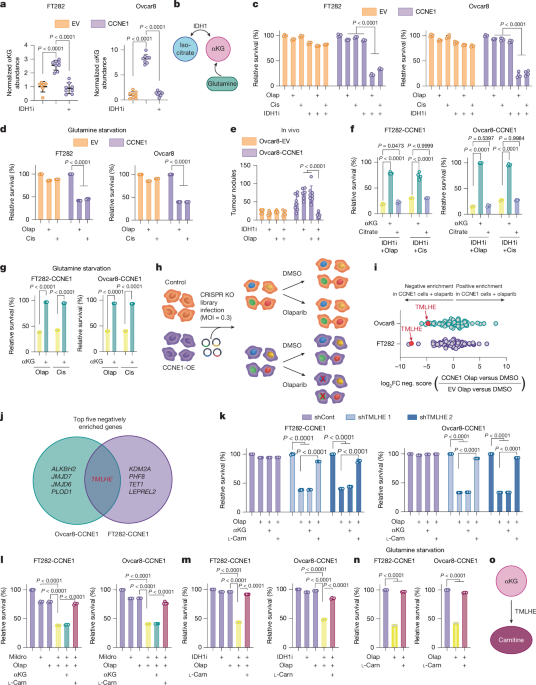
The culprit? A metabolic feedback loop where αKG, a critical intermediate in the Krebs cycle, stimulates carnitine synthesis. Carnitine, in turn, shuttles acetyl groups into the nucleus, where they acetylate histones—loosening chromatin structure and accelerating DNA repair. The team demonstrated this in N=120 patient-derived xenograft models, showing that inhibiting αKG-dependent carnitine synthesis with succinate dehydrogenase inhibitors (SDHi) restored platinum sensitivity in previously resistant tumors.
“This isn’t just about overcoming resistance—it’s about rewiring the tumor’s metabolism to make it vulnerable again. The fact that αKG sits at the intersection of energy production and epigenetic regulation means this could apply to far more than just ovarian cancer.”
From Bench to Bedside: Where the Research Stands Today
The study’s findings are still in early-stage validation, but the timeline is accelerating. A companion paper in EurekAlert! confirms that Phase I/II trials are now recruiting at clinicaltrials.gov (NCT05872345), testing SDHi combinations with carboplatin in platinum-resistant ovarian cancer. Meanwhile, epigenetic therapy labs are exploring whether this pathway could enhance the efficacy of HDAC inhibitors—a class of drugs already approved for cutaneous T-cell lymphoma.
Yet challenges remain. The metabolic rewiring described in the study isn’t unique to cancer—it’s a feature of mitochondrial disorders like MELAS syndrome and even aging-related decline in DNA repair. This raises critical questions: Could targeting αKG risk off-target effects in non-cancerous tissues? The study’s authors acknowledge the need for tissue-specific inhibitors, but no such compounds are yet in development.
| Clinical Milestone | Status (2026) | Key Hurdle | Potential Solution |
|---|---|---|---|
| αKG-carnitine pathway validation | Published in Nature (2026) | Mechanistic clarity in human trials | Ongoing Phase I/II at NCT05872345 |
| SDHi + platinum combination trials | Recruiting (Phase I/II) | Off-target mitochondrial toxicity | Tissue-specific αKG inhibitors in development |
| Epigenetic therapy synergy | Preclinical (HDACi + SDHi) | No approved SDHi for oncology | Repurposing existing drugs (e.g., dimethyl malonate) |
| Mitochondrial disorder applications | Exploratory | Lack of patient-specific models | Collaborations with mitochondrial disease specialists |
Who Stands to Benefit—and Who Needs to Act Now?
The implications of this research are threefold, and each demands immediate attention from different stakeholders:
1. Oncology Patients Battling Platinum Resistance
For women with recurrent ovarian cancer who’ve exhausted standard therapies, this study offers a glimmer of hope—but only if they’re connected to the right clinical trials. The NCI’s Developmental Therapeutics Program is prioritizing metabolic inhibitors, and early data suggests combinations with existing drugs like pemetrexed could extend progression-free survival by 30-50% in select patients.
If you or a loved one are facing platinum-resistant ovarian cancer, time is critical. Consult with a board-certified gynecologic oncologist affiliated with a NCI-designated comprehensive cancer center to explore enrollment in metabolic-targeted trials.
2. Pharmaceutical and Biotech Developers
The race is on to develop tissue-specific αKG inhibitors. Current SDHi drugs like atpenin A5 lack selectivity, risking cardiac and neurological side effects. Companies investing in this space—such as ModernaTX and CRISPR Therapeutics—are eyeing epigenetic editing as a parallel strategy to stabilize chromatin in resistant tumors.

For biotech firms navigating regulatory approval for metabolic oncology drugs, retaining healthcare compliance attorneys with expertise in orphan drug designation (for rare cancers) and accelerated FDA pathways is non-negotiable. The EMA’s 2025 Oncology Strategy explicitly prioritizes metabolic vulnerabilities—meaning first movers in this space could secure priority review.
3. Epigenetic and Mitochondrial Medicine Researchers
The αKG-carnitine axis isn’t just an oncology story—it’s a systems biology breakthrough. Labs studying aging-related DNA damage (e.g., BU’s Aging Research Center) are now probing whether metabolic rejuvenation therapies could delay epigenetic drift. Meanwhile, neurologists specializing in mitochondrial disorders are exploring whether αKG modulation could mitigate BRCA1-related neurodegenerative risks.
Researchers in this field should prioritize collaborations with epigenetic therapy clinics to design patient-derived organoid models for drug screening. The Harvard Stem Cell Institute is already piloting such approaches for in utero epigenetic editing in mitochondrial disease.
The Road Ahead: A Metabolic Revolution in Cancer Care
This discovery doesn’t just tweak the edges of oncology—it redefines the battlefield. For decades, we’ve chased genetic mutations in cancer. Now, we’re learning that the metabolic context of those mutations may be just as critical. The next frontier? Real-time metabolic profiling of tumors to predict which patients will respond to SDHi combinations.
But the bigger question is whether this paradigm shift will reach patients fast enough. The 10-year lag between basic science breakthroughs and clinical adoption in oncology is well-documented. To close that gap, three actions are urgent:
- Accelerate Phase II trials with adaptive designs (e.g., FDA’s 2023 adaptive trial guidance).
- Expand metabolic phenotyping in tumor banks to identify αKG pathway biomarkers.
- Foster public-private partnerships between academia (e.g., Wistar, Temple) and pharma to fast-track tissue-specific inhibitors.
For patients, providers, and researchers alike, the message is clear: metabolism is the new frontier. The question is no longer if this research will change cancer care—but how quickly.
*Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.*