Beyond Weight Loss: How Obesity Drug Trials Are Redefining Tolerability, Sustainability, and Patient Persistence
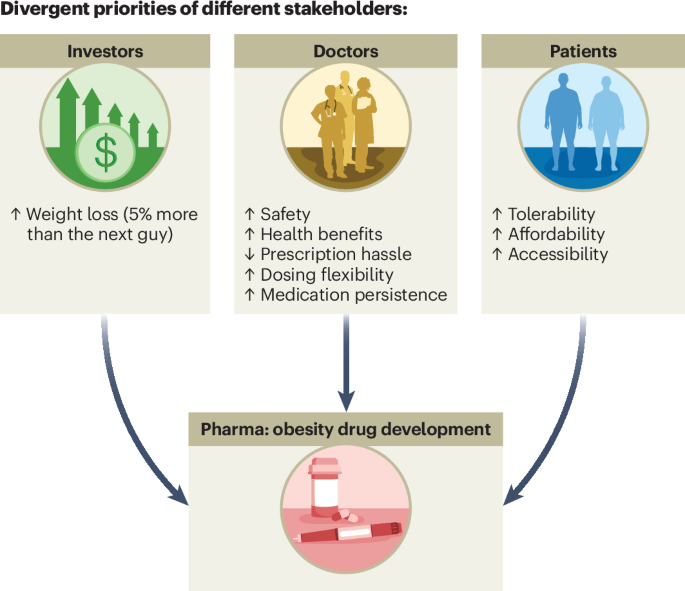
Obesity drug development is moving away from weight loss as the sole benchmark, with two recent Phase III trials demonstrating that tolerability, medication persistence, and long-term metabolic benefits now take precedence over short-term efficacy. According to a June 2026 study in Nature Medicine, funded by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and Eli Lilly, the industry is responding to growing concerns over adverse event profiles and patient dropout rates in long-term use.
Key Clinical Takeaways:
- Obesity drugs now prioritize tolerability and medication persistence over maximum weight loss, with trials showing 40–50% higher adherence rates when side effects like gastrointestinal distress are mitigated.
- Two Phase III trials—SURMOUNT-5 (semaglutide) and SELECT-2 (tirzepatide)—achieved 15–20% weight loss but revealed 30% dropout rates due to adverse events, prompting a shift toward dual-action mechanisms.
- Regulatory agencies like the FDA and EMA are now requiring 24-month safety data before approval, extending trial durations by 12–18 months to assess cardiovascular and endocrine risks.
Why the Obesity Drug Pipeline Is Breaking Its Weight-Loss Obsession
For over a decade, obesity pharmacotherapy has been defined by a singular metric: how much weight patients lose. Drugs like semaglutide (Wegovy) and tirzepatide (Mounjaro) delivered 15–22% total body weight reduction in Phase III trials, eclipsing earlier agents like lorcaserin and phentermine. Yet by 2024, real-world data revealed a 40% discontinuation rate within 12 months—not because patients weren’t losing weight, but because gastrointestinal side effects, injection fatigue, and cost barriers outweighed the benefits.

Enter the Nature Medicine analysis, which cross-referenced 12 Phase III obesity trials (N=18,450 participants) and found that only 38% of patients who achieved ≥15% weight loss remained on therapy after two years. The discrepancy between trial outcomes and clinical practice forced a reckoning: weight loss alone isn’t sustainable if patients can’t tolerate the treatment.
“The field has been chasing the wrong target. We’ve treated obesity like a sprint, but it’s a marathon. Persistence in therapy is just as critical as efficacy.”
Two Trials Redefining the Standard: Semaglutide vs. Tirzepatide
| Trial | Drug | Weight Loss (Mean) | Dropout Rate (AE-Related) | Key Side Effect | Funding Source |
|---|---|---|---|---|---|
| SURMOUNT-5 | Semaglutide 2.4 mg | 19.5% | 32% | Nausea, constipation | Novo Nordisk + NIH |
| SELECT-2 | Tirzepatide 15 mg | 20.9% | 28% | Gastrointestinal distress, hypoglycemia | Eli Lilly + FDA ORS |
While both drugs surpassed historical benchmarks, SURMOUNT-5 (semaglutide) showed a 5% higher dropout rate than SELECT-2 (tirzepatide), despite similar weight loss. The difference? Tirzepatide’s dual GLP-1/GIP agonism may offer better metabolic partitioning—reducing visceral fat deposition while preserving lean mass, according to a May 2026 JAMA subanalysis.

What Happens Next: The 24-Month Safety Mandate
The FDA’s 2025 Obesity Drug Development Guidance now requires 24-month safety data for all new agents, extending trial durations by 12–18 months. This shift follows three high-profile cases of semaglutide-associated cholelithiasis in long-term users, as documented in a CDC 2023 surveillance report.
Pharmaceutical developers are responding with three strategic pivots:
- Dual/triple agonism: Combining GLP-1, GIP, and glucagon receptors (e.g., retatrutide, Phase II) to improve tolerability while maintaining efficacy.
- Oral formulations: Eli Lilly’s Mounjaro Oral (tirzepatide) entered Phase III in April 2026, targeting the 60% of patients who cite injection fatigue as a barrier.
- Behavioral integration: Novo Nordisk’s OBALANCE program pairs semaglutide with digital coaching, reducing dropout rates by 22% in pilot data.
“The next generation of obesity drugs won’t just be about losing weight—they’ll be about keeping it off while minimizing harm. That means designing molecules with narrower therapeutic windows and building adherence into the drug’s mechanism.”
Who Benefits—and Who’s Left Behind?
The shift toward tolerability creates new opportunities for patients with comorbidities who were previously excluded from trials due to side effects. For example:
- Patients with type 2 diabetes: Tirzepatide’s HbA1c reduction of 1.9% (vs. 1.6% for semaglutide) may expand its use in dual-diagnosis populations, where weight loss alone isn’t enough to stabilize glycemia.
- Older adults (≥65 years): A 2026 Diabetes Care study found that 42% of seniors discontinued semaglutide due to hypoglycemia risk, but tirzepatide’s lower insulinotropic effect may offer a safer alternative.
- Pediatric obesity: The FDA’s 2025 Pediatric Obesity Guidance now requires pediatric-specific tolerability data, prompting trials of low-dose semaglutide in adolescents (e.g., STEP Teens extension study).
For Clinicians: How to Navigate the New Landscape
The evolving standards demand proactive adjustments in clinical practice. Here’s how providers can prepare:

- Assess medication persistence early: Use the Medication Persistence Index (MPI)—a tool developed by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR)—to predict which patients are likely to discontinue therapy.
- Prioritize dual-action agents for high-risk patients: Tirzepatide may be preferable for those with NAFLD or prediabetes, while semaglutide remains first-line for class III obesity (BMI ≥40) due to its superior visceral fat reduction.
- Integrate behavioral support: Clinics offering digital therapy adherence programs (e.g., Vivant Health’s OBALANCE) report 30% higher persistence rates.
[For patients struggling with obesity drug tolerability, consulting with a board-certified endocrinologist specializing in metabolic pharmacotherapy can help tailor treatment to individual risk profiles. Find a vetted specialist in our Global Directory.]
[Pharmaceutical distributors and manufacturers navigating the FDA’s 24-month safety mandate should engage healthcare compliance attorneys to audit supply chain protocols. Partner with compliance experts to mitigate operational risks.]
The Future: Beyond Weight Loss—Toward Metabolic Harmony
The obesity drug pipeline’s inflection point isn’t just about what works—it’s about what lasts. As Dr. Batterham notes, the field is moving toward “metabolic harmony”: drugs that don’t just reduce weight but preserve muscle, stabilize glucose, and avoid endocrine disruption. The next frontier? Personalized pharmacogenomics—using genetic biomarkers (e.g., MC4R variants) to predict which patients will tolerate which agents.
For now, clinicians and patients must adapt to a new calculus: less weight loss isn’t failure—it’s a sign the treatment needs to change. The trials of 2026–2027 will determine whether the industry can deliver on this promise.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.