AI Prioritization of Chest X-rays: No Impact on Lung Cancer Diagnosis Speed – A Large UK Study
AI Prioritization Fails to Accelerate Lung Cancer Diagnosis, Major UK Trial Finds
A large-scale, randomized trial involving nearly 100,000 patients has found that using artificial intelligence to prioritize chest X-rays did not significantly speed up the lung cancer diagnostic pathway, according to results published today in Nature Medicine. The study, led by researchers at University College London Hospitals (UCLH), University College London (UCL), and the University of Nottingham, casts doubt on the immediate benefits of deploying AI for this purpose, despite its increasing adoption in healthcare settings.
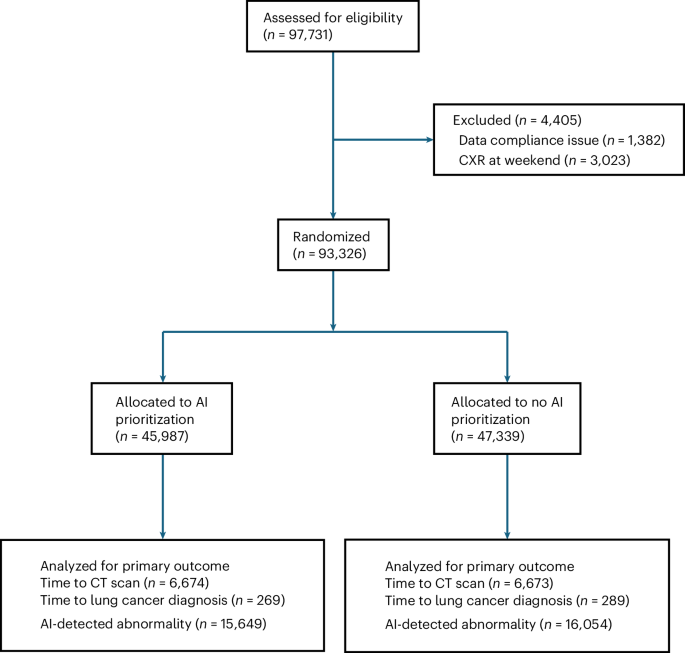
The LungIMPACT trial, conducted across five NHS trusts in England, examined whether immediately flagging potentially cancerous findings on chest X-rays (CXRs) with AI would lead to faster computed tomography (CT) scans and diagnoses. Researchers found no significant difference in the median time to CT scans – 53 days with AI prioritization versus 53 days without – or the time to lung cancer diagnosis, which was 44 days and 46 days respectively. The difference in diagnosis time was not statistically significant.
While the AI system did reduce the time it took for a radiologist to initially report on a chest X-ray, from 47 hours to 34 hours, this improvement did not translate into faster overall progress through the diagnostic process. “The bottleneck isn’t the reporting; it’s everything that happens next: telling the patient, the CT appointment, the clinic slot, the multidisciplinary meeting,” explained UCLH consultant radiographer and principal investigator Nick Woznitza. “We’ve shown that AI prioritization, by itself, cannot fix that.”
The study analyzed 93,326 CXRs, with 13,347 leading to CT scans and 558 resulting in a lung cancer diagnosis. Researchers also examined discordance rates between the AI’s findings and those of radiologists, finding discrepancies in 28,261 CXRs (approximately 30 percent). Analysis of these discrepancies revealed that AI flagged potential issues in 11.6 percent of cases that were ultimately deemed false positives by radiologists.
The findings raise questions about the cost-effectiveness of implementing AI prioritization systems, particularly given the “considerable and avoidable” costs associated with their installation and maintenance. A detailed health economics evaluation is forthcoming, according to the study authors. The research also highlights systemic challenges within the NHS, including limited CT scanner availability and shortages of radiologists and radiographers, which may hinder the ability to rapidly respond to AI-identified abnormalities.
The National Institute for Health and Care Excellence (NICE) has not recommended any AI products for CXR interpretation in England, reflecting concerns about their efficacy and potential for unintended consequences. Researchers noted the risk of “vigilance fatigue,” where radiologists may become desensitized to AI-flagged abnormalities or lose trust in the system’s accuracy over time.
The study’s strength lies in its randomized controlled design and large sample size, minimizing the potential for bias. Researchers also conducted extensive discordance reviews, providing a large dataset for analyzing the accuracy of the AI system. However, the study focused on a single AI product, and its findings may not be generalizable to all AI algorithms. The study did not evaluate the impact of AI in conjunction with other pathway changes, such as mandated immediate radiologist review of all AI-prioritized scans.
A separate study, currently underway in Glasgow, Scotland, is assessing the impact of AI prioritization on time to CT among patients with suspected lung cancer. The results of that trial are expected to provide further insight into the potential benefits and limitations of this technology.
The LungIMPACT trial concludes that, in its current implementation, AI prioritization of CXRs does not offer a significant advantage in accelerating lung cancer diagnosis within the English NHS. The research team suggests that focusing on addressing systemic bottlenecks in the diagnostic pathway may be a more effective approach to improving outcomes for patients with suspected lung cancer.