
Unveiling Insights into Pulmonary Arterial hypertension: A Deep Dive into Study Populations and Biomarker Analysis
Pulmonary Arterial Hypertension (PAH) is a progressive and debilitating disease characterized by increased pressure in the pulmonary arteries, leading to right heart failure and reduced quality of life. Recent research, detailed in a study published in Nature, has focused on identifying biomarkers that can aid in diagnosis, prognosis, and possibly, the advancement of targeted therapies. This article provides a extensive overview of the study’s methodology, specifically focusing on the meticulous design of patient cohorts and the rigorous analytical techniques employed to assess the role of Notch3 extracellular domain (NOTCH3-ECD) as a potential biomarker for IPAH.
Study Populations and Sample Collection: A Multi-Center Approach
The study employed a robust design, incorporating both cross-sectional and longitudinal cohorts to provide a comprehensive understanding of NOTCH3-ECD levels in relation to IPAH. Between 2010 and 2021, researchers prospectively collected serum samples from a total of 717 individuals – 341 diagnosed with Idiopathic PAH (IPAH) and 376 without PAH. These participants were recruited from three prominent medical centers: the University of California, San Diego (UCSD), the University of Arizona (Phoenix), and Massachusetts General Hospital (Boston).
Cross-Sectional Cohorts: Establishing Baseline Differences
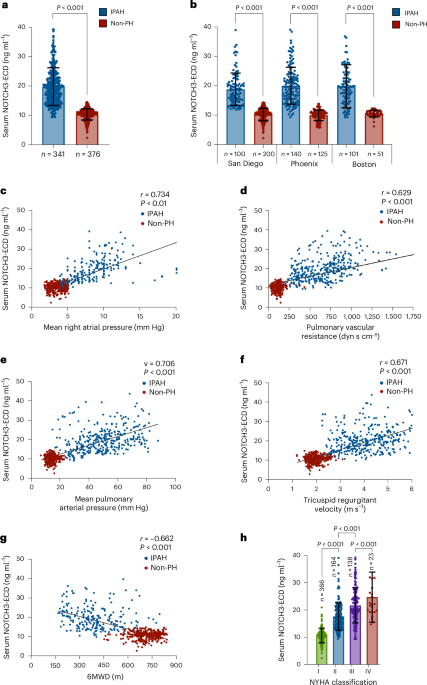
The cross-sectional analysis involved the following cohort breakdowns:
- San Diego: 100 IPAH patients, 200 non-PH controls
- Phoenix: 140 IPAH patients, 125 non-PH controls
- Boston: 101 IPAH patients, 51 non-PH controls
A key aspect of the study design was the statistical power calculation. Researchers resolute that a sample size of 341 IPAH patients and 376 non-PH individuals would provide 90% power to detect a minimum effect size of 0.27 for differences in serum NOTCH3-ECD levels between the two groups, using a two-sided alpha level of 0.05. This rigorous approach ensures the reliability and validity of the findings.
The collection methods varied slightly between sites. San Diego and Phoenix collected samples from outpatients, while Boston collected samples from patients hospitalized in the ICU due to IPAH. Informed consent was obtained from all participants, and patient sex was recorded as assigned at the time of hospital admission. All IPAH blood samples were collected within one month of a Right Heart Catheterization (RHC) or Echocardiogram (ECHO), standard diagnostic procedures for assessing pulmonary hypertension.
Control groups were carefully selected. In San Diego and phoenix, healthy, paid volunteers served as controls. The Boston cohort comprised ICU patients *without* PAH, who were being treated for non-lung-related conditions.This group included patients with orthopedic trauma, post-operative recovery, head injuries, and amyotrophic lateral sclerosis. All participants underwent RHC as part of the study protocol.Importantly, all IPAH patients tested negative for HIV, active hepatitis, and a comprehensive panel of autoimmune antibodies, minimizing the influence of confounding factors.
To ensure a focused study, patients with subtypes of PAH linked to known causes (heritable mutations, methamphetamine use, scleroderma, HIV, congenital heart defects, portal hypertension, or pulmonary veno-occlusive disease) were excluded from the primary analysis. However, samples from these patients were collected for secondary comparative analyses. Additionally, samples were collected from individuals with non-PH vasculitides and malignancies expressing NOTCH3, further broadening the scope of inquiry.
Longitudinal Cohort: Tracking Changes over Time
To assess the dynamic changes in NOTCH3-ECD levels and their correlation with disease progression,a separate longitudinal cohort of 100 newly diagnosed,treatment-naive IPAH patients was established. This cohort comprised 43 patients from San Diego and 57 from Phoenix. These patients were followed for six years, with serial blood samples collected alongside ECHO and RHC data at diagnosis, three years, and six years. This longitudinal design allows researchers to track the evolution of NOTCH3-ECD levels in relation to clinical outcomes.
Sample Collection and Processing: Ensuring Data Integrity
Blood samples were collected via venipuncture into heparin-coated tubes and processed to separate serum using Ficoll gradient centrifugation. Serum samples were then stored at -80°C and de-identified using a barcode system to maintain patient confidentiality. For a subset of ten patients, serum was obtained directly from the pulmonary artery and left atrium during cardiac catheterization, providing insights into the origin of NOTCH3-ECD.
All studies received approval from the relevant Institutional Review Boards (IRBs), including those at UCSD, Mass General Brigham, the University of Arizona, and others, ensuring ethical conduct and patient safety. The study also adhered to guidelines outlined in the UK National Cohort Study of Idiopathic and Heritable Pulmonary Arterial Hypertension (ClinicalTrials.gov ID: NCT01907295).
NOTCH3-ECD Quantification: ELISA Methodology
Serum levels of NOTCH3-ECD were quantified using a commercially available Enzyme-Linked Immunosorbent Assay (ELISA) kit (Cloud Clone, cat. no. SEL147Hu). The ELISA was performed according to the manufacturer’s protocol, with operators blinded to the case/control status of the samples to minimize bias. A series of NOTCH3-ECD standards were used to establish a concentration curve, and samples were diluted 1:5 before analysis. each sample was tested in triplicate to ensure accuracy and reproducibility. Absorbance was measured using a SpectraMax M2e plate reader, and data were analyzed using SoftMax Pro v5.4.
Ensuring Specificity: Cross-Reactivity Testing
To confirm the specificity of the ELISA, researchers tested for cross-reactivity with recombinant human NOTCH1-ECD, NOTCH2-ECD, and NOTCH4-ECD. This step is crucial to ensure that the assay is specifically detecting NOTCH3-ECD and not other related proteins.
Validating Results: Immunoprecipitation and Western Blotting
Immunoprecipitation and Western blotting were performed to further validate the ELISA findings and confirm the presence of NOTCH3-ECD in serum samples. These techniques provide complementary evidence supporting the ELISA results.
Statistical Analysis: Rigorous Evaluation of data
The study employed a range of statistical methods to analyze the data. Logistic regression and Receiver Operating Characteristic (ROC) curves were used to assess the ability of NOTCH3-ECD levels to differentiate between IPAH patients and controls. The optimal cutoff value for NOTCH3-ECD was determined using Youden’s Index and the F1 score. Kaplan-Meier plots and Cox proportional hazards models were used to evaluate the prognostic value of NOTCH3-ECD levels in predicting mortality.
To further refine risk prediction, machine learning models, specifically XGBoost, were employed, incorporating NOTCH3-ECD levels alongside established risk scores like REVEAL 2.0, REVEAL 2.0 Lite, and COMPERA 2.0. This approach aimed to improve the accuracy of predicting 3-year mortality in IPAH patients.
Statistical meaning was set at p < 0.05. Data were analyzed using GraphPad Prism and R software.
Addressing Missing Data
The study acknowledged the presence of a small amount of missing data (3.5-5% in the cross-sectional cohort and 2-3% in the longitudinal cohort). However, no imputation methods were used, and data were analyzed as available.
Conclusion: Advancing the Understanding of IPAH
This comprehensive study provides valuable insights into the potential role of NOTCH3-ECD as a biomarker for IPAH. The meticulous design of the patient cohorts, rigorous analytical techniques, and robust statistical analysis contribute to the strength of the findings. The integration of machine learning models further enhances the potential for improved risk stratification and personalized medicine approaches in the management of this challenging disease. Further research is warranted to validate these findings in larger, autonomous cohorts and to explore the therapeutic implications of targeting the NOTCH3 pathway in IPAH.