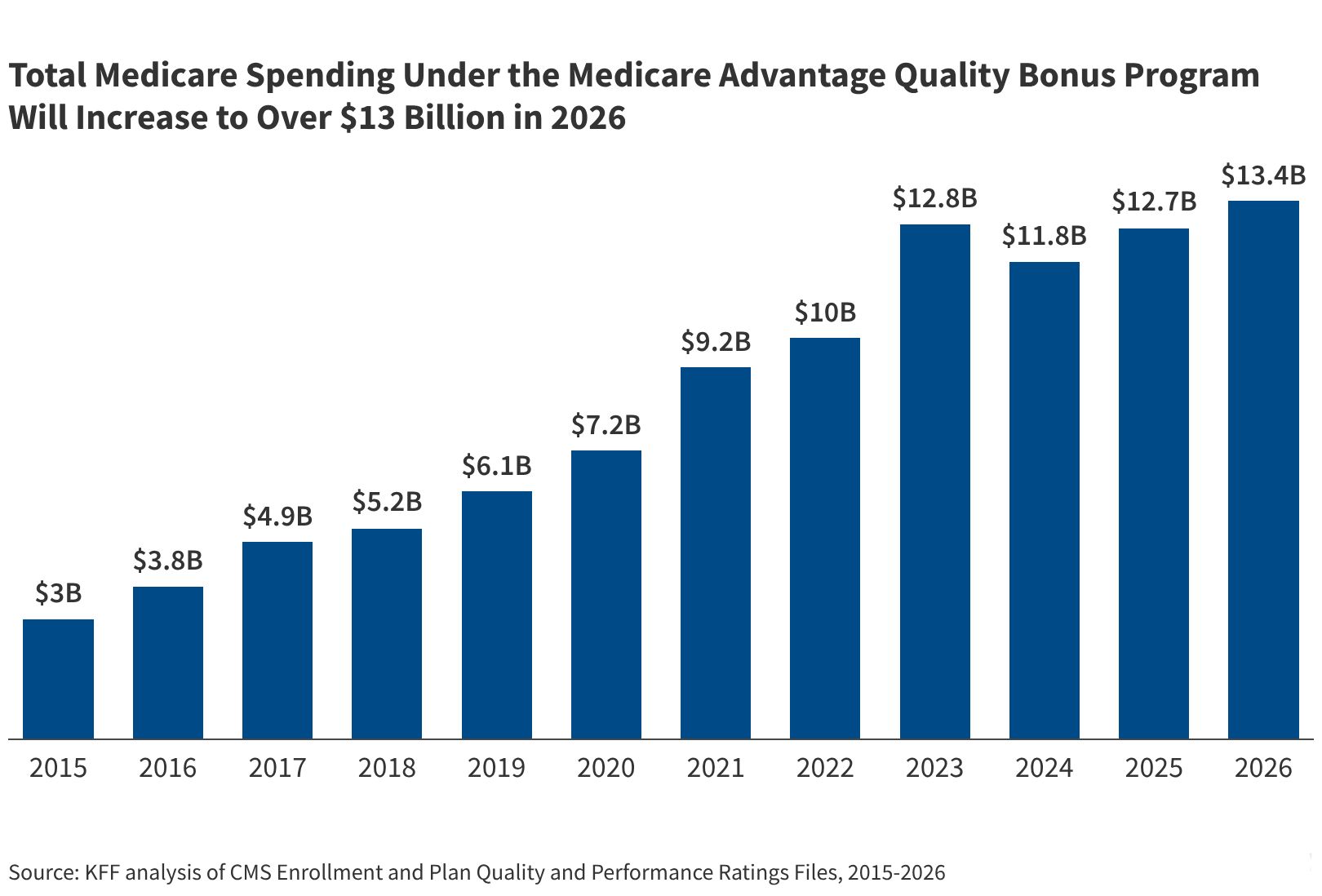
Medicare Advantage Quality Bonus Spending to Hit $13 Billion in 2026
The Medicare program will spend at least $13 billion on the Medicare Advantage quality bonus program in 2026, according to government data, as 68% of Medicare Advantage enrollees are now in plans qualifying for higher payments. This expenditure reflects the scaling of the Quality Bonus Payment (QBP) system, which rewards plans that meet specific star-rating thresholds for clinical performance and patient satisfaction.
- Fiscal Impact: Medicare spending on quality bonuses will exceed $13 billion in 2026.
- Enrollment Shift: Nearly 70% of Medicare Advantage members are in high-performing, bonus-eligible plans.
- Payment Mechanism: Bonuses are tied to star ratings, influencing how the government reimburses private insurers.
The surge in spending highlights a systemic shift in how the Centers for Medicare & Medicaid Services (CMS) incentivizes private insurers. By tying financial rewards to quality metrics, the government aims to reduce morbidity and improve the standard of care. However, the concentration of enrollees in bonus-eligible plans creates a significant budgetary requirement for the federal government, as these payments are added to the base per-member per-month (PMPM) rates.
For healthcare organizations and private practices, this financial structure influences the types of care delivery models they encounter. Organizations seeking to optimize their reimbursement cycles or align with high-performing plans often require the guidance of [Healthcare Compliance Attorneys] to ensure that clinical documentation supports the quality metrics required for these bonuses.
Why is the Medicare Advantage quality bonus spending increasing?
The increase is driven by a high percentage of enrollees moving into plans that have achieved the necessary star ratings to qualify for the QBP. According to the CMS framework, plans that earn a 4-star rating or higher receive a bonus payment. Because 68% of the population is currently enrolled in such plans, the aggregate payout has reached the $13 billion threshold for the 2026 cycle.
This mechanism is designed to encourage “value-based care,” a model that prioritizes patient outcomes over the volume of services provided. In clinical terms, this means a focus on reducing the pathogenesis of chronic complications through better preventative screenings and medication adherence. When a plan successfully manages a population’s hypertension or diabetes, the star rating rises, triggering the bonus.
The financial incentive structure is analyzed in depth by the Centers for Medicare & Medicaid Services (CMS), which oversees the administration of these payments. The objective is to create a competitive environment where insurers compete on the quality of care provided to the beneficiary.
How do quality bonuses affect clinical outcomes for patients?
The quality bonus program relies on a set of HEDIS (Healthcare Effectiveness Data and Information Set) measures and CAHPS (Consumer Assessment of Healthcare Providers and Systems) surveys. These metrics track critical health indicators, such as the percentage of patients receiving annual wellness visits or the rate of colorectal cancer screenings. By rewarding plans that hit these targets, CMS effectively pushes insurers to mandate more rigorous preventative care protocols.

However, the transition to these models can create gaps in care if the focus shifts too heavily toward “gaming” the metrics rather than holistic patient health. For patients with complex comorbidities—such as those managing both end-stage renal disease and congestive heart failure—the standard of care must extend beyond the checkboxes of a star rating. Patients requiring specialized, high-acuity interventions are encouraged to seek [Specialized Diagnostic Centers] to ensure that their complex needs are met with precision medicine rather than generalized plan protocols.
According to data available via PubMed, the correlation between high star ratings and actual clinical health outcomes is a subject of ongoing longitudinal study. While higher ratings generally align with better preventative care, the actual reduction in long-term morbidity varies across different demographic cohorts.
What are the regulatory implications for 2026 and beyond?
The $13 billion expenditure represents a significant portion of the Medicare Advantage budget, leading to increased scrutiny from federal auditors and the Office of Inspector General (OIG). The primary concern is whether the bonus payments are providing a genuine return on investment in the form of improved public health or if they are simply inflating the profit margins of private insurers.
This regulatory environment necessitates a high level of transparency in how “quality” is defined. If CMS adjusts the star-rating methodology—as it has done in previous years to make it more difficult to achieve a 5-star rating—the number of eligible plans could drop, potentially reducing the total bonus payout in future years. Such shifts in federal policy require immediate operational pivots for medical groups. Providers who rely on the stability of these payments often consult with [Medical Billing and Revenue Cycle Management Services] to hedge against potential reimbursement volatility.
The broader impact of these payments is often compared to the benchmarks set by the World Health Organization (WHO) regarding universal health coverage and quality standards. The U.S. model of using private bonuses to drive public health outcomes is a distinct approach compared to the single-payer systems seen in other developed nations.
The trajectory of value-based reimbursement
The 2026 spending projection confirms that the Medicare Advantage quality bonus program is no longer a niche incentive but a core component of the U.S. healthcare financial architecture. As the program expands, the focus will likely shift from simple preventative measures to more complex outcome-based metrics, such as the reduction of hospital readmission rates and the integration of behavioral health into primary care.

For the medical community, the challenge remains the alignment of financial incentives with the actual needs of the patient. While $13 billion in bonuses suggests a success in plan performance, the ultimate metric of success is the lived experience of the enrollee. To ensure that care remains patient-centric amidst these financial shifts, it is essential for beneficiaries to utilize vetted, board-certified specialists who prioritize clinical evidence over plan-driven metrics.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.