
This text discusses the management and causes of Torsades de Pointes (TdP),a potentially life-threatening heart rhythm. Here’s a breakdown of the key data:
Causes of Acquired QT Interval Prolongation (leading to TdP):
Drug-induced: Many medications can prolong the QT interval. The text lists a wide range of drug classes, including:
Class 1A and Class III antiarrhythmics (e.g., quinidine, procainamide, amiodarone, sotalol)
antihistamines (e.g., terfenadine, astemizole)
Macrolide antibiotics (e.g., erythromycin, clarithromycin, azithromycin)
Pentamidine
Serotonin receptor antagonists (e.g., ketanserin)
Diuretics (e.g., indapamide)
Certain fluoroquinolone antibiotics
Tricyclic antidepressants
Antipsychotics (e.g., phenothiazines, haloperidol, thioridazine)
gastrointestinal motility enhancers (e.g., cisapride, domperidone)
Inotropes (e.g., amrinone, milrinone)
Antimalarials (e.g., chloroquine, hydroxychloroquine)
Methadone
Electrolyte derangements:
Hypomagnesemia (low magnesium)
Hypokalemia (low potassium)
Hypocalcemia (low calcium)
Toxins: Organophosphates, arsenic.
Management of Torsades de Pointes:
Immediate Treatment:
Discontinue offending medications: If drug-induced arrhythmias are suspected, any QT-prolonging medications should be stopped.
Intravenous Magnesium Sulfate: This is the initial therapy, nonetheless of serum magnesium levels. A 2-g bolus is followed by an infusion of 2-4 mg/min.
Pharmacologic Approaches (when initial therapy is insufficient or for specific situations):
Beta-blockade: While not a first-line approach to acutely terminate TdP, it’s part of managing arrhythmic storm. Nonselective beta-blockers (like propranolol) are preferred, ofen combined with IV amiodarone in patients with structural heart disease and electrical storm, unless contraindicated. Lidocaine: A Class IB antiarrhythmic that blocks sodium currents and can shorten the QTc interval. It’s included in some guidelines and can be considered if beta-blockers and amiodarone are ineffective. It’s also beneficial for cardiac arrest due to shock-refractory VF or polymorphic VT.
Avoid certain medications: Amiodarone and procainamide,which prolong the QT interval,should not be used for tdp or arrhythmic storm associated with a prolonged QT,as they can worsen the condition.
monitoring: Patients requiring potentially arrhythmia-inducing drugs should have regular ECGs and othre tests based on their profile and the drug’s characteristics.
Long-term Management and Prevention:
Implantable Cardioverter-Defibrillators (ICDs): For patients susceptible to TdP and other ventricular arrhythmias.
Complete medical strategies.
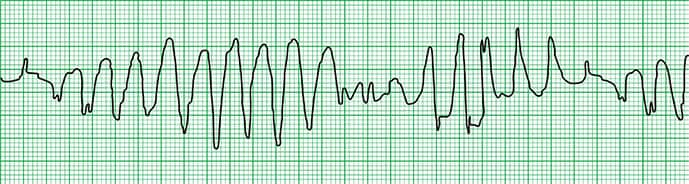
Key Takeaways from the Case Illustration:
The case highlights a likely drug-induced TdP from methadone in the presence of electrolyte abnormalities.
It emphasizes the importance of evaluating for potential cardiogenic causes of syncope (fainting) in patients with abnormal ECGs.
Critically important Note: The text mentions that the article was created using generative AI models as part of the process, with human review and editing.