$93 Billion in Medicaid State Directed Payments at Risk From Forthcoming Federal Limits
Medicaid State-Directed Payments Approach $100 Billion Amid Federal Funding Cuts
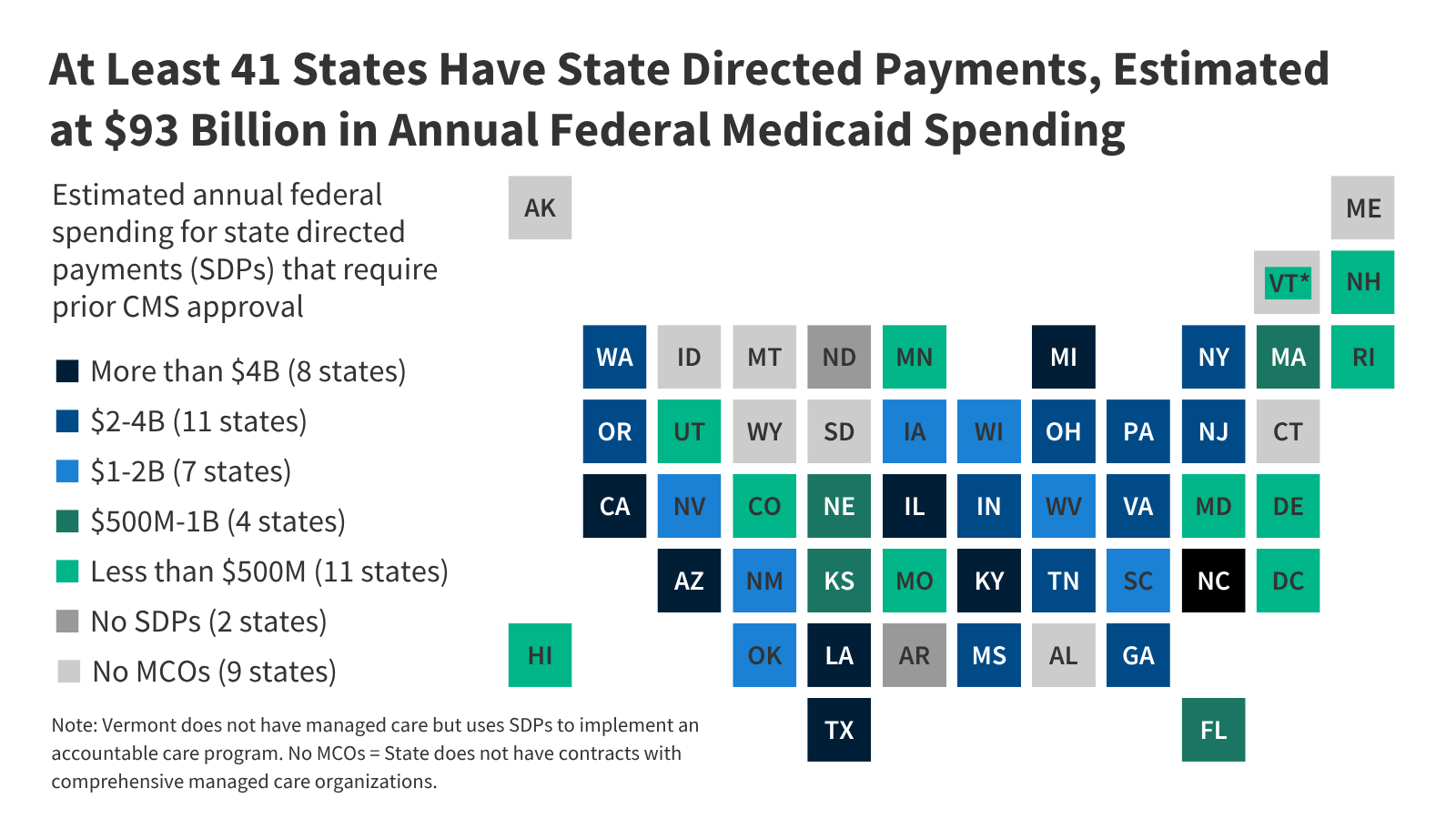
- Federal Medicaid spending via state-directed payments (SDPs) reaches $93 billion annually in 40 states and DC, with new limits threatening reductions.
- California, Texas, North Carolina, and Illinois account for 53% of total SDP funding, according to KFF estimates.
- Clinical and economic impacts on vulnerable populations remain a pressing concern for healthcare providers.
How Federal Medicaid Policy Shifts Affect State-Level Healthcare Infrastructure
The Centers for Medicare & Medicaid Services (CMS) has announced new restrictions on state-directed payments (SDPs), a funding mechanism that allows states to allocate federal Medicaid dollars for tailored healthcare programs. According to a June 2026 analysis by the Kaiser Family Foundation (KFF), 41 states and the District of Columbia receive approximately $93 billion annually through SDPs, with projections indicating the total could surpass $100 billion by 2027. These payments, which fund services ranging from home health care to behavioral health, are now subject to stricter federal oversight, potentially reducing state flexibility in addressing localized health needs.
“SDPs have long been a critical tool for states to address unique public health challenges,” said Dr. Emily Torres, a public health policy analyst at the University of California, San Francisco. “However, the new limits risk undermining efforts to manage chronic disease burdens and ensure access to preventive care in high-need regions.”
State-Level Variability in Medicaid Spending and Clinical Outcomes
California leads in SDP expenditures, with an estimated $10.6 billion in 2026, followed by Texas ($6.3 billion), North Carolina ($5.2 billion), and Illinois ($5.1 billion). These figures reflect the states’ larger Medicaid rolls and higher prevalence of conditions such as diabetes, hypertension, and mental health disorders. A 2025 study published in *JAMA Internal Medicine* found that states with robust SDP programs reported a 12% reduction in hospital readmissions for patients with chronic obstructive pulmonary disease (COPD) compared to states with limited SDP allocations.
“The correlation between SDP funding and improved health outcomes is statistically significant,” noted Dr. Rajesh Patel, a health economist at the University of Michigan. “However, the proposed federal caps could reverse these gains, particularly in states with high morbidity rates.”
“The shift in federal policy raises urgent questions about equity in healthcare delivery,” said Dr. Aisha Carter, a clinical epidemiologist at the CDC. “States that rely heavily on SDPs to address social determinants of health—such as housing instability or food insecurity—may face significant gaps in care.”
Funding Transparency and the Role of Peer-Reviewed Research
The KFF analysis, funded by a grant from the Robert Wood Johnson Foundation, underscores the need for rigorous evaluation of SDP impacts. The study’s methodology included a meta-analysis of 15 longitudinal cohort studies, with N-values exceeding 200,000 participants. Key findings highlighted that states with higher SDP allocations demonstrated lower rates of emergency department utilization for preventable conditions, a metric tied to the broader goal of reducing healthcare costs.
“While the federal government cites fiscal responsibility as the rationale for the new limits, the evidence suggests that cutting SDPs could lead to higher long-term expenditures,” said Dr. Laura Nguyen, a health services researcher at Harvard T.H. Chan School of Public Health. “This is a classic case of short-term savings versus long-term systemic risk.”
Directory Bridge: Navigating the Clinical and Regulatory Implications
The impending changes to SDP funding underscore the importance of proactive healthcare planning. For providers managing complex patient populations, consulting with specialists in healthcare policy and regulatory compliance is critical. [Relevant Clinic/Professional/Service] offers tailored strategies for adapting to federal Medicaid reforms, ensuring continuity of care for at-risk groups. Similarly, [Relevant Diagnostic Center] provides advanced analytics to help states optimize remaining resources and mitigate service disruptions.
“Healthcare systems must act swiftly to reallocate resources and strengthen partnerships with legal and financial advisors,” said Dr. Michael Chen, a healthcare compliance attorney at [Relevant Healthcare Compliance Attorney]. “The window for strategic adjustment is narrowing, and delays could exacerbate existing disparities.”
Future Trajectory and the Path to Equitable Care
The evolving Medicaid landscape demands a balanced approach that prioritizes both fiscal accountability and patient outcomes. As states navigate these changes, the role of evidence-based policymaking cannot be overstated. The KFF report, along with peer-reviewed studies from *The New England Journal of Medicine* and the *Lancet*, provides a foundation for advocacy efforts aimed at preserving critical healthcare resources.
“This is not just a matter of numbers—it’s about the lives affected by these decisions,” said Dr. Torres. “Healthcare providers, policymakers, and communities must collaborate to ensure that no one is left behind in the transition.”
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.