US Public Support for Global Health Aid Declines
The stability of global health is not a charitable luxury but a clinical necessity. When the infrastructure of international health surveillance collapses, the biological distance between a remote outbreak and a domestic clinic vanishes, leaving healthcare systems vulnerable to pathogens that do not recognize national borders.
Key Clinical Takeaways:
- A majority of the public anticipates that the dissolution of USAID will result in increased illness and death within low-income nations.
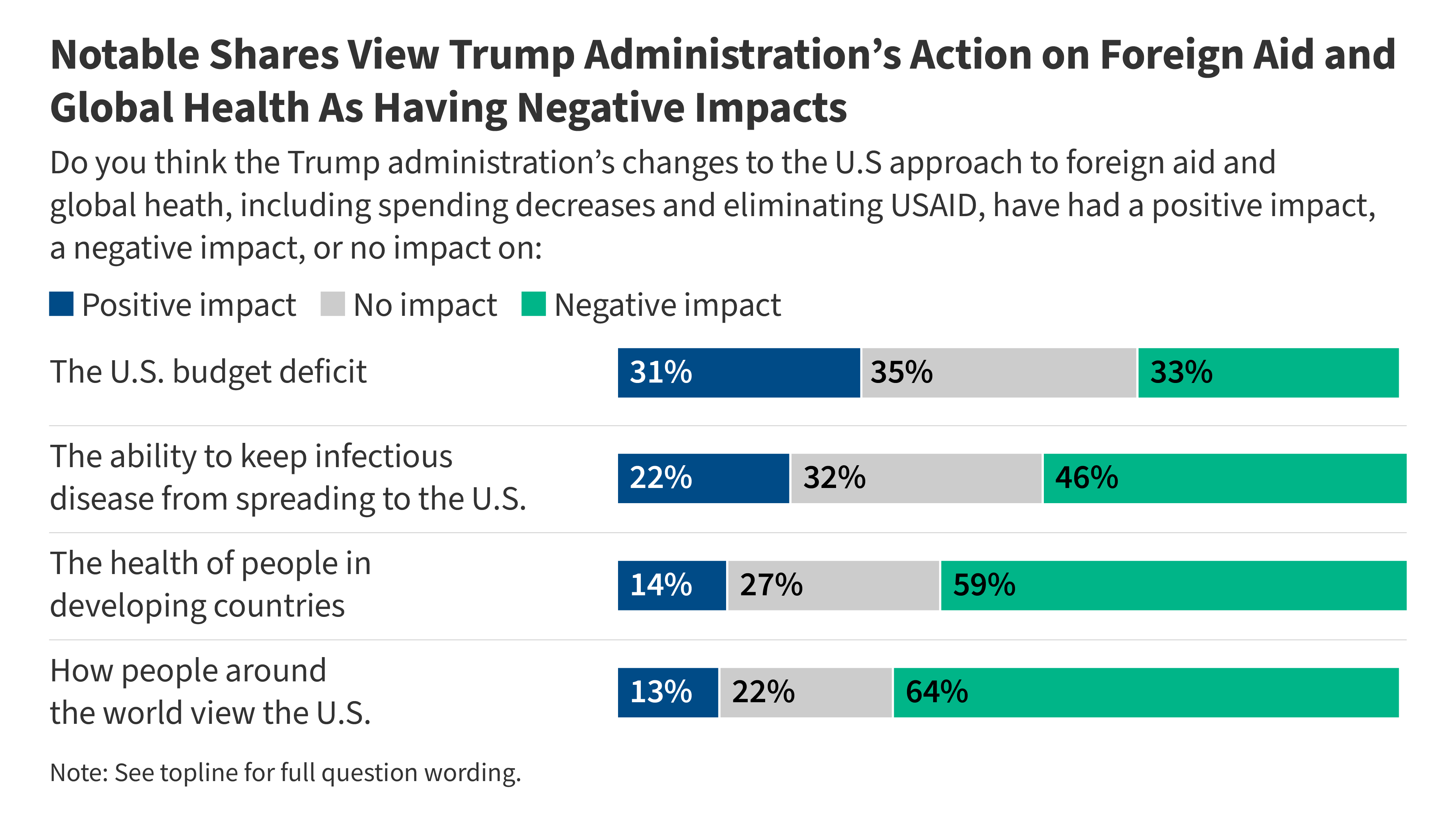
- Public opinion is sharply divided, with nearly half of respondents viewing the redirection of foreign aid as a viable path to reducing the U.S. Budget deficit.
- Despite fiscal concerns, only 13% of adults support the total elimination of U.S. Foreign aid.
The recent KFF Health Tracking Poll February 2025 illuminates a profound tension between domestic fiscal policy and global epidemiological security. As the Trump administration moves to dissolve the U.S. Agency for International Development (USAID) and freeze the majority of foreign aid—including critical global health funding—the American public is grappling with the potential clinical fallout. The data reveals a stark reality: 67% of adults believe that eliminating USAID is likely to lead to more illness and death in low-income countries, while 62% expect an increase in global humanitarian crises.
From a clinical perspective, this funding vacuum creates an environment ripe for the acceleration of antimicrobial resistance (AMR) and the unchecked spread of zoonotic diseases. Global health funding often supports the “standard of care” in regions where the pathogenesis of infectious diseases is most volatile. When these programs are defunded, the result is not merely a loss of aid but a breakdown in epidemiological surveillance. Without the ability to track viral mutations or manage bacterial outbreaks in real-time, the global community loses its early warning system, increasing the statistical probability of a pandemic that could bypass domestic containment efforts.
“The removal of coordinated global health funding creates ‘blind spots’ in our planetary surveillance. When we stop monitoring disease vectors in developing regions, we aren’t saving money; we are essentially outsourcing the next pandemic’s incubation period to the most vulnerable populations.”
The risk is not limited to viral outbreaks. The erosion of global health infrastructure directly impacts the management of chronic morbidity and the delivery of essential vaccines. The dissolution of USAID threatens the supply chains for life-saving medications, which can lead to incomplete treatment cycles. In the case of tuberculosis or malaria, inconsistent medication adherence is a primary driver of drug-resistant strains. These “superbugs” eventually migrate, necessitating more aggressive and expensive interventions for patients in the U.S. To manage the resulting complexity of imported drug-resistant infections, hospitals are increasingly relying on board-certified infectious disease specialists to implement strict antimicrobial stewardship protocols.
The KFF poll highlights a significant ideological split regarding the utility of these funds. Approximately 47% of respondents believe that removing USAID will allow funds to be redirected toward domestic programs, and another 47% suggest it will significantly reduce the U.S. Budget deficit. This reflects a “zero-sum” perception of healthcare spending. However, the clinical reality is that global health security is a form of preventative medicine on a planetary scale. The cost of maintaining a functional USAID is a fraction of the economic and clinical cost associated with a single uncontrolled global health emergency.
For the organizations and private entities currently operating in the international health space, this shift in federal policy creates an immediate regulatory and operational crisis. NGOs and pharmaceutical partners who relied on USAID grants must now navigate a precarious funding landscape while attempting to maintain the continuity of care for millions. This volatility requires a rigorous audit of contractual obligations and a strategic pivot in funding models. Many of these organizations are now retaining healthcare compliance attorneys to manage the transition and ensure that the cessation of federal funds does not lead to legal liabilities or a total collapse of essential medical services.
The biological implications of this policy shift extend to the very concept of “One Health”—the integrated approach that recognizes the interconnection between people, animals, and their shared environment. Much of the funding provided via USAID supports the monitoring of animal-to-human spillover events. Without this oversight, the window between the emergence of a new pathogen and its detection widens. For domestic health systems, this means a shorter reaction time to implement triage and containment. This increased risk profile makes the role of professional epidemiologists critical in developing domestic contingency plans that can compensate for the loss of international data streams.
While 13% of the public supports the total elimination of foreign aid, the overwhelming majority recognizes that some level of engagement is necessary. The challenge lies in balancing the perceived need for domestic fiscal austerity with the objective clinical risk of global health instability. The history of public health demonstrates that isolationism is an ineffective strategy against microscopic threats. Pathogens do not adhere to budget cuts or political mandates; they follow the path of least resistance provided by weakened healthcare infrastructures.
As we move further into 2026, the medical community must prepare for the tangible effects of these funding gaps. The shift from a proactive, funded global surveillance model to a reactive, domestic-only model increases the morbidity risk for populations worldwide and introduces systemic vulnerabilities into the U.S. Healthcare apparatus. The future of global health will likely depend on whether private philanthropy and international coalitions can fill the void left by the U.S. Government, or if the world will enter a period of heightened epidemiological fragility.
Maintaining clinical excellence in this uncertain environment requires access to vetted, high-authority medical expertise. Whether navigating the complexities of emerging infectious diseases or managing the legal ramifications of shifting health policies, utilizing a verified directory of professionals is the most reliable way to ensure patient safety and operational continuity.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.