US Parasite Outbreak: Why Explosive Diarrhea Cases Are Hard to Contain
Public health authorities are currently managing a surge in cyclosporiasis cases across multiple U.S. states, a parasitic infection triggered by the protozoan Cyclospora cayetanensis. The infection, characterized by acute, explosive diarrhea and severe gastrointestinal distress, is frequently linked to the consumption of contaminated fresh produce. Clinical teams are now tasked with identifying these cases amidst a broader landscape of seasonal enteric pathogens, necessitating high-index suspicion to prevent protracted patient morbidity.
Key Clinical Takeaways:
- Cyclosporiasis is a foodborne illness caused by Cyclospora cayetanensis, typically presenting with watery, explosive diarrhea, fatigue, and abdominal cramping.
- The current standard of care for confirmed cases is a combination of trimethoprim-sulfamethoxazole (TMP-SMX), though clinical management often requires specialized diagnostic stool testing due to the parasite’s intermittent shedding patterns.
- Public health surveillance is actively identifying transmission clusters, with individuals experiencing persistent gastrointestinal symptoms advised to seek immediate consultation with [Board-Certified Gastroenterologists] for definitive stool ova and parasite (O&P) examination.
Epidemiological Mechanisms and Pathogenesis
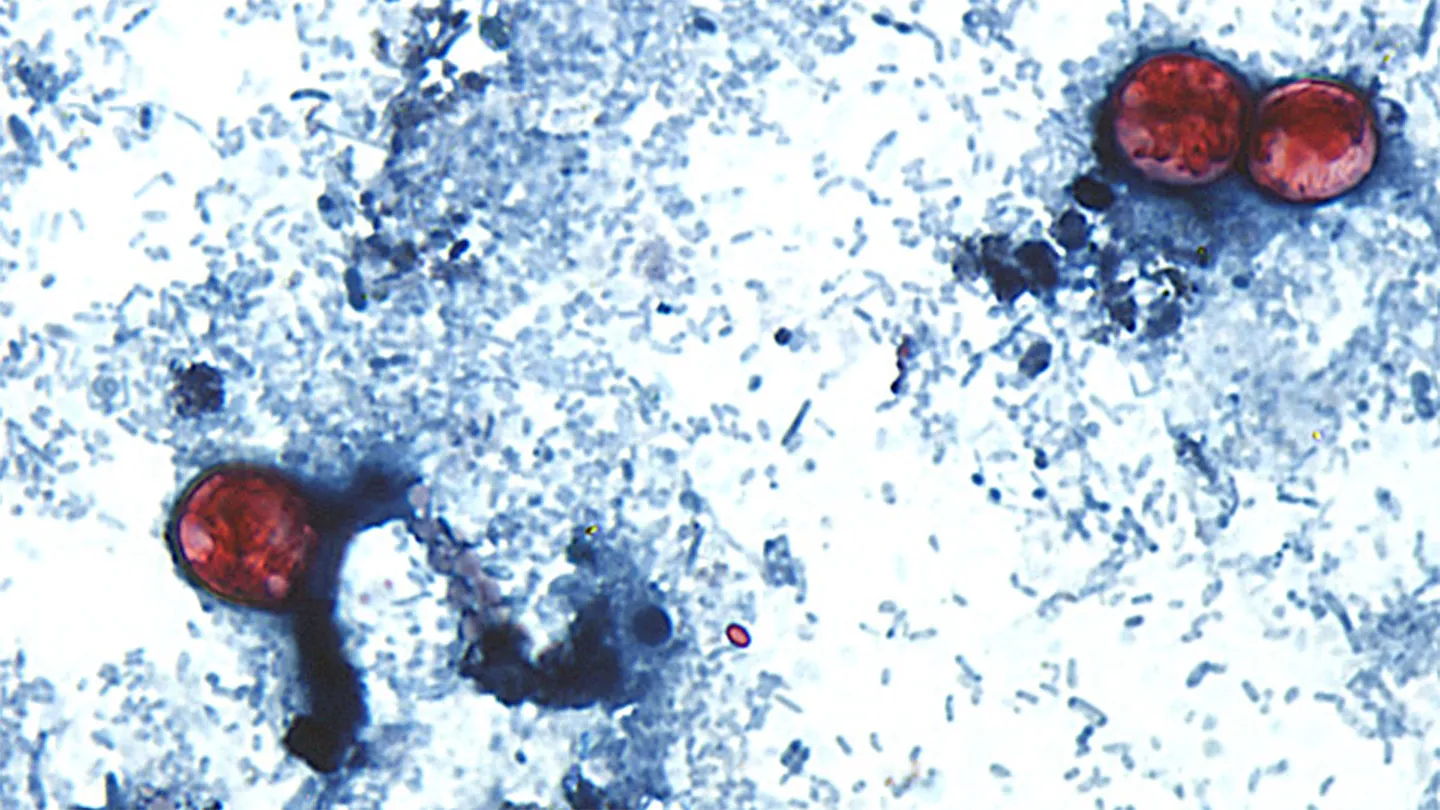
The pathogenesis of Cyclospora cayetanensis begins upon the ingestion of sporulated oocysts, typically through contaminated water or raw agricultural products. Once ingested, the oocysts excyst in the upper small intestine, invading the epithelial cells. This intracellular cycle leads to villous atrophy and crypt hyperplasia, which disrupts normal absorption and results in the hallmark watery diarrhea. According to data published by the Centers for Disease Control and Prevention (CDC), the incubation period is approximately one week, though symptoms can persist for several weeks or even months if left untreated.
The diagnostic challenge remains significant. Because Cyclospora oocysts are not consistently present in every stool sample, clinicians are urged to order multiple specimens collected on different days to increase diagnostic sensitivity. Advanced molecular diagnostics, including polymerase chain reaction (PCR) panels, are increasingly utilized to differentiate Cyclospora from other common enteric pathogens like Giardia or Cryptosporidium. For clinical labs and diagnostic centers facing high testing volumes, maintaining rigorous quality control is essential; practitioners should consult with [Accredited Diagnostic Laboratory Services] to ensure their protocols meet current CDC surveillance standards.
Clinical Management and Therapeutic Protocols
The primary clinical intervention for symptomatic cyclosporiasis is the administration of trimethoprim-sulfamethoxazole (TMP-SMX). Clinical research, including studies supported by the National Institute of Allergy and Infectious Diseases (NIAID), emphasizes that antibiotic resistance is not currently a widespread concern, but patient adherence to the full treatment course is critical to preventing relapse. For patients with documented sulfa allergies, alternative therapeutic options remain limited, often requiring off-label management strategies developed in consultation with infectious disease specialists.
“The primary issue with Cyclospora is the delay in diagnosis,” notes Dr. Elena Rodriguez, an infectious disease epidemiologist. “Patients often cycle through multiple primary care visits, receiving symptomatic treatment for presumed viral gastroenteritis, before a stool O&P or molecular panel is performed. This delay not only exacerbates patient suffering but also hinders public health efforts to identify the contaminated food source.”
Public Health Surveillance and Regulatory Oversight
Containing the current outbreak requires close coordination between the Food and Drug Administration (FDA) and state health departments. The FDA’s ongoing investigations into food supply chains are funded through federal appropriations dedicated to food safety and outbreak response. When a cluster is identified, the traceability of fresh produce—such as cilantro, basil, or imported berries—becomes the focal point of the epidemiological investigation.
For healthcare providers and food safety officers, navigating the reporting requirements during an active outbreak is a complex administrative burden. Organizations involved in the distribution and retail of fresh produce are increasingly retaining [Healthcare and Regulatory Compliance Attorneys] to ensure adherence to FDA food safety modernization protocols and to mitigate the risks of operational disruption during product recalls.
Future Trajectories in Enteric Pathogen Research
As the frequency of Cyclospora outbreaks appears to fluctuate with seasonal agricultural imports, the focus of clinical research is shifting toward more rapid, point-of-care molecular diagnostic tools. Reducing the time-to-diagnosis from days to hours is the next frontier in minimizing community transmission. Clinicians are encouraged to maintain a high index of suspicion for patients presenting with prolonged diarrheal illness, particularly during the summer months. To ensure your practice or facility is equipped with the latest diagnostic standards and referral pathways, we recommend reviewing the vetted resources available via our [Global Medical Specialist Directory].
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.