US and Global Fund Funding Cuts Analysis 2026-2029: Impact on 29 Countries
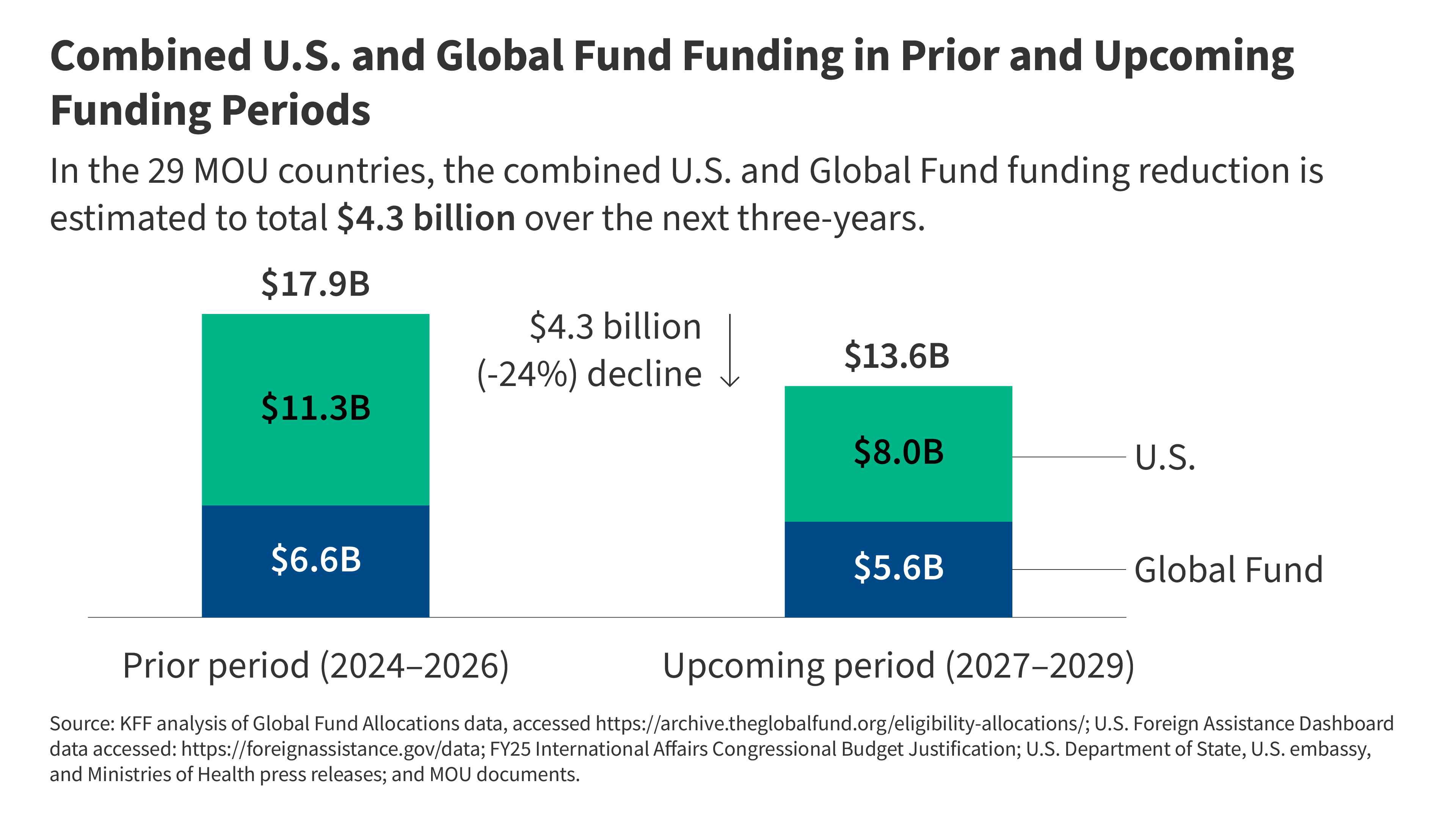
Significant reductions in financial commitments from the United States government and the Global Fund to Fight AIDS, Tuberculosis and Malaria are projected to impact 29 countries with active Memoranda of Understanding (MOU) between 2026 and 2029. This fiscal contraction, driven by shifting budgetary priorities in donor nations and revised internal allocation models, threatens the continuity of essential public health programs, including antiretroviral therapy (ART) distribution and vector-borne disease control, according to recent budgetary analysis released by the Global Fund’s Secretariat.
Key Clinical Takeaways:
- Fiscal retrenchment threatens to disrupt the standard of care for HIV, TB, and malaria in 29 high-burden nations through 2029.
- Reductions in external funding necessitate a rapid pivot toward domestic resource mobilization and optimized supply chain efficiency to prevent a surge in disease-related morbidity.
- Healthcare systems must immediately integrate diagnostic and therapeutic protocols to mitigate the risks associated with treatment interruptions and potential drug resistance.
Epidemiological Risks of Funding Contraction
The reduction in international health financing creates a tangible risk of treatment default. In HIV management, the clinical standard of care requires uninterrupted adherence to antiretroviral therapy to maintain viral suppression and prevent the emergence of drug-resistant viral strains. Data published in The Lancet Infectious Diseases suggests that even brief interruptions in therapy can lead to rapid viral rebound, increasing the risk of opportunistic infections and community-level transmission. When funding for diagnostic testing and pharmaceutical procurement decreases, the probability of undiagnosed or untreated cases rises, potentially reversing decades of progress in lowering population-level morbidity.

“The stability of global health security is intrinsically linked to the predictability of multi-year funding cycles. A sudden withdrawal of support in high-burden regions does not merely slow progress; it actively risks the re-emergence of pathogens that we have spent years bringing under clinical control,” notes Dr. Elena Rossi, an infectious disease epidemiologist and independent health systems consultant.
Clinical Triage and Resource Optimization
As public health infrastructure faces these fiscal headwinds, healthcare providers are increasingly required to prioritize high-yield interventions. The shift necessitates a transition from broad-based outreach to targeted clinical screening. For regional clinics attempting to maintain service levels, the integration of advanced diagnostic tools is essential to ensure that limited pharmaceutical supplies are directed toward patients with the highest clinical need. Facilities facing supply chain volatility should engage with accredited diagnostic centers to streamline screening protocols and minimize wastage.
Furthermore, the administrative burden of managing reduced budgets while maintaining clinical compliance is substantial. Hospitals and non-governmental organizations are currently seeking guidance to ensure that institutional changes do not fall below the World Health Organization guidelines for care. For those managing complex institutional transitions, consulting with healthcare compliance attorneys is a proactive measure to ensure that cost-cutting measures remain within the bounds of international medical law and patient rights frameworks.
Comparative Analysis of Funding Trajectories
The following table outlines the anticipated impact of funding shifts on core clinical domains, based on projections derived from the Centers for Disease Control and Prevention (CDC) global health budget outlook and Global Fund replenishment reports.

| Clinical Domain | Primary Risk Factor | Clinical Consequence |
|---|---|---|
| HIV/AIDS | ART Supply Disruption | Viral rebound and drug resistance |
| Tuberculosis | Diagnostic screening gaps | Increased transmission of MDR-TB |
| Malaria | Vector control reduction | Seasonal morbidity spikes |
Future Trajectory and Clinical Resilience
The long-term success of health programs in MOU-impacted countries now depends on the rapid scaling of domestic financing and private-sector partnerships. Clinical research indicates that countries with robust, diversified funding models are better equipped to withstand external shocks. However, the transition period remains precarious. Physicians and public health administrators must remain vigilant in monitoring patient outcomes and maintaining the integrity of treatment regimens despite systemic resource limitations. Maintaining access to specialized care and expert guidance remains a critical component of managing these risks. Providers and administrators are encouraged to coordinate with vetted public health consultants to optimize resource allocation and ensure the continuity of essential services during this period of fiscal uncertainty.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.