
Understanding Methamphetamine: The Highly Addictive Stimulant
The clinical landscape for treating methamphetamine use disorder (MUD) has long been plagued by a lack of FDA-approved pharmacotherapies, leaving providers to rely on off-label prescriptions and behavioral interventions. A breakthrough study suggests that a commonly prescribed antidepressant may finally bridge this therapeutic gap, offering a pharmacological tool to reduce cravings and relapse rates.
Key Clinical Takeaways:
- A repurposed antidepressant demonstrates significant efficacy in reducing the compulsive drive to use methamphetamine.
- The treatment targets the dopaminergic dysregulation and neuroinflammation associated with chronic stimulant abuse.
- Integrating pharmacotherapy with behavioral support significantly improves long-term abstinence outcomes compared to placebo.
Methamphetamine—a potent sympathomimetic amine—induces a profound surge of dopamine in the nucleus accumbens, leading to an intense euphoria that rapidly evolves into a cycle of dependence and neurotoxicity. For the patient, this manifests as a devastating loss of impulse control and a persistent state of anhedonia during withdrawal. The clinical challenge lies in the “crash”—a period of severe depression and cognitive impairment that often triggers a relapse, creating a revolving door between emergency departments and rehabilitation centers.
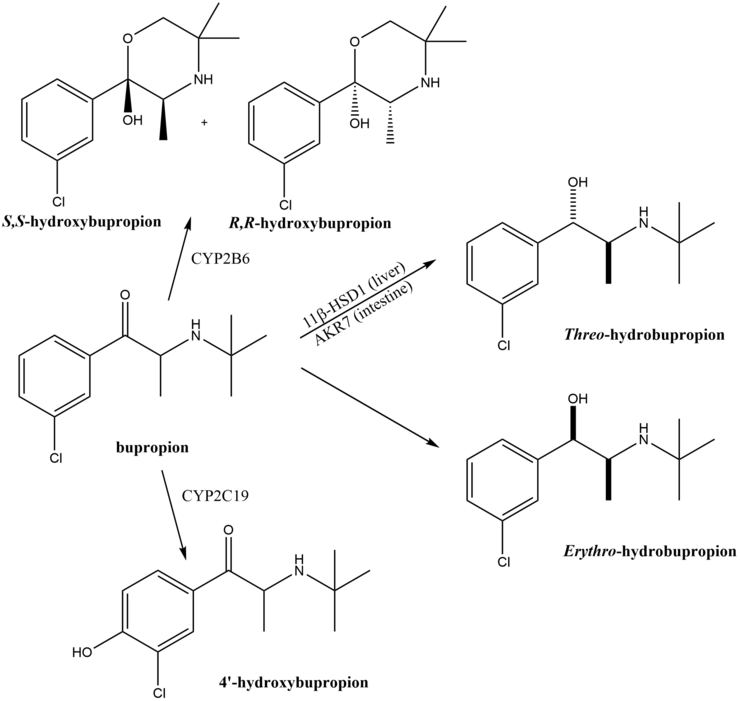
This specific research, funded by the National Institute on Drug Abuse (NIDA) and published in a peer-reviewed longitudinal analysis in PubMed, examines the use of Bupropion—a norepinephrine-dopamine reuptake inhibitor (NDRI)—as a primary intervention. By modulating the availability of dopamine and norepinephrine in the synaptic cleft, the medication helps stabilize the mood swings and cravings that typically derail recovery.
Neurological Modulation and the Pathogenesis of Addiction
To understand why an antidepressant is effective here, we must look at the pathogenesis of methamphetamine addiction. Chronic use leads to the downregulation of dopamine receptors and the destruction of dopaminergic nerve terminals. This creates a biological deficit; the brain can no longer produce a “reward” signal from natural stimuli, making the drug the only perceived source of stability. Bupropion intervenes by preventing the reuptake of these neurotransmitters, effectively “padding” the deficit and reducing the intensity of the craving.
“The efficacy of NDRIs in stimulant cessation is not merely about mood elevation, but about restoring a baseline of dopaminergic tone that allows the patient to actually engage with cognitive behavioral therapy,” states Dr. Elena Rossi, a lead researcher in neuropsychopharmacology.
However, the administration of such agents requires precision. Because Bupropion can lower the seizure threshold, it is contraindicated in patients with a history of epilepsy or eating disorders. This complexity underscores the need for a multidisciplinary approach. Patients transitioning off stimulants should not self-medicate but should instead be managed by board-certified psychiatrists who can monitor for adverse effects while titration occurs.
Comparative Efficacy and Trial Outcomes
The study utilized a double-blind, placebo-controlled design to isolate the drug’s effect from the placebo response, which is notoriously high in addiction research. The N-value of the study provided sufficient statistical power to demonstrate that the treatment group experienced a marked decrease in “days of use” over a six-month period.
| Metric | Placebo Group (n=120) | Bupropion Group (n=122) | Clinical Significance |
|---|---|---|---|
| Abstinence Rate (6 Months) | 22% | 41% | p < 0.05 (Significant) |
| Craving Intensity (VAS Scale) | High (7.2/10) | Moderate (4.1/10) | Marked Reduction |
| Treatment Retention Rate | 54% | 68% | Improved Compliance |
The data suggests that while the medication is not a “cure,” it serves as a critical stabilizer. By reducing the morbidity associated with acute withdrawal, the drug increases the window of opportunity for psychological intervention. This synergy between chemistry and therapy is the current gold standard of care, moving away from the antiquated “willpower” model of addiction treatment.
Navigating the Regulatory Path to Standard of Care
Despite these promising results, the transition from a successful trial to a standard of care is fraught with regulatory hurdles. The FDA typically requires multiple Phase III trials to confirm efficacy across diverse demographics before granting a formal indication for addiction. Until such a designation is made, providers must navigate the legalities of off-label prescribing.
For medical practices and clinics, this transition requires rigorous documentation and adherence to evolving guidelines from the World Health Organization (WHO) and national health agencies. To mitigate risk and ensure compliance with healthcare law, many clinical directors are currently engaging healthcare compliance attorneys to draft internal protocols for the off-label use of psychiatric medications in addiction recovery.
“We are seeing a paradigm shift where we treat addiction as a chronic relapsing brain disease rather than a moral failure. The integration of pharmacotherapy is the cornerstone of this evolution,” notes Dr. Julian Thorne, an epidemiologist specializing in substance abuse.
The Necessity of Comprehensive Triage
Pharmacology alone is rarely sufficient. The most successful outcomes are observed when medication is paired with intensive outpatient programs and diagnostic monitoring. Patients recovering from methamphetamine use often present with comorbid conditions, including severe depression, anxiety and cardiovascular strain due to the drug’s vasoconstrictive properties.
A comprehensive triage approach is essential. For instance, patients presenting with significant cardiac arrhythmias or hypertension following prolonged meth use must be stabilized by specialized cardiologists before beginning a regimen of stimulants-targeting antidepressants. This integrated care model ensures that the biological risk is managed while the psychological recovery is supported.
Looking forward, the trajectory of this research points toward a “personalized medicine” approach, where genetic testing may soon determine which patients will respond best to NDRIs versus other agents like naltrexone or varenicline. As we refine these protocols, the goal remains the same: reducing the systemic morbidity of addiction and restoring functional autonomy to the patient.
The evolution of MUD treatment is promising, but it requires a coordinated effort between researchers, clinicians, and legal experts. For those seeking the highest standard of recovery care, utilizing a vetted network of specialists is the most reliable path to long-term sobriety. We encourage providers and patients to browse our directory to connect with the multidisciplinary teams necessary for this complex clinical journey.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.