The Trump administration is temporarily halting some Medicaid funding to Minnesota, citing concerns over fraud, Vice President JD Vance announced Wednesday. The move, which will initially withhold at least $515 million each quarter, marks a significant escalation in the administration’s scrutiny of state Medicaid programs and a departure from previous federal practices.
Vance, speaking alongside Administrator for the Centers for Medicare & Medicaid Services (CMS) Dr. Mehmet Oz, described the action as part of an “aggressive crackdown on misuse of public funds.” The administration alleges non-compliance with federal requirements designed to prevent fraud, waste and abuse within Minnesota’s Medicaid program.
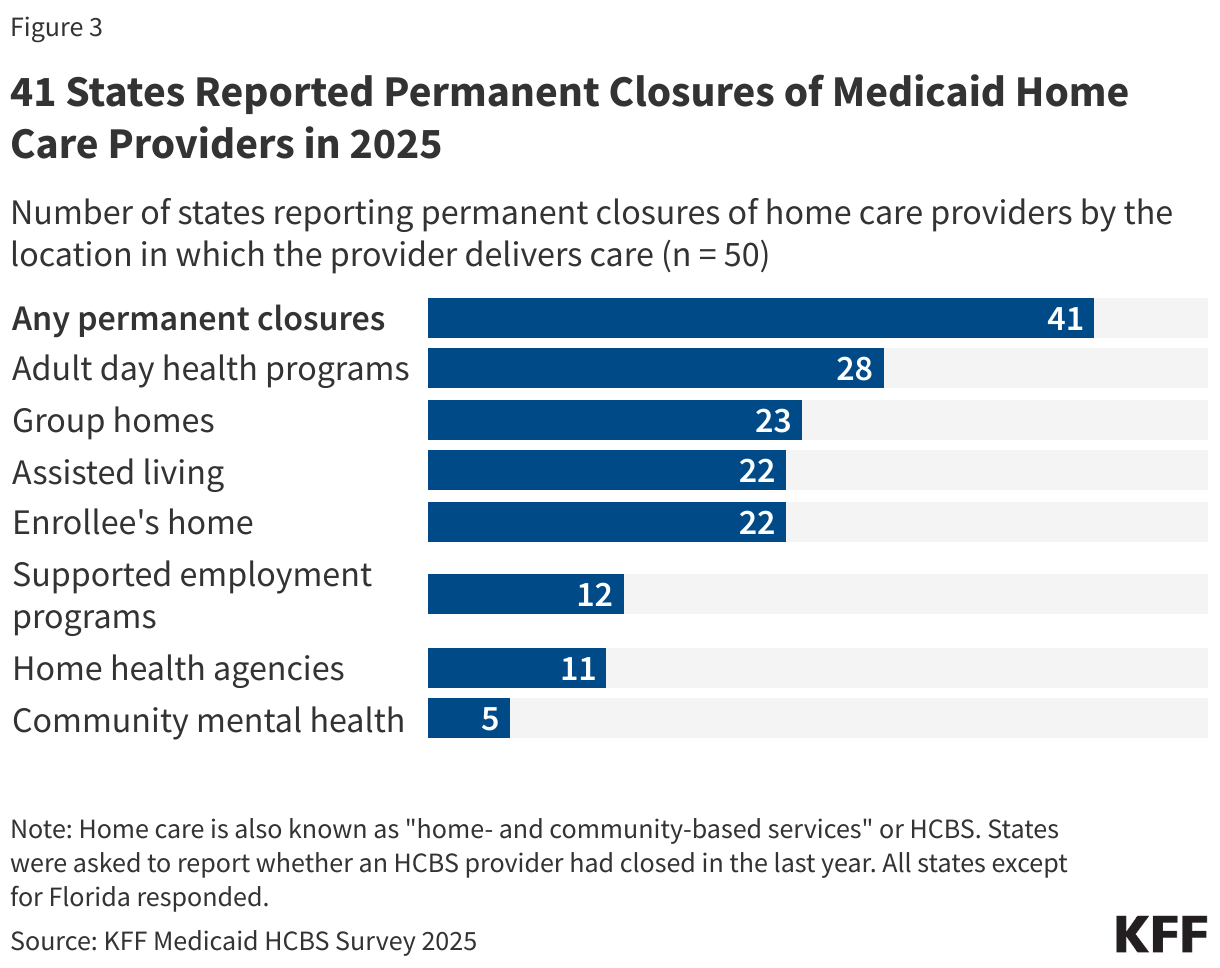
The concerns center on alleged fraud within Minnesota’s Medicaid home care programs, which provide assistance with daily living activities to older adults and people with disabilities. These programs have grown significantly in recent years, with over 5 million people nationally now utilizing Medicaid home care, according to estimates from the Kaiser Family Foundation (KFF). The administration’s focus on home care reflects a broader concern about potential vulnerabilities in this sector, where services are delivered in private homes to individuals who may be less able to advocate for themselves.
CMS issued a letter to Minnesota Governor Tim Waltz on February 14, 2026, outlining the alleged deficiencies and initiating the funding pause. The agency rejected an initial corrective action plan submitted by the state within a week, and Minnesota is currently appealing that decision even as submitting a revised plan on January 30, 2026.
Minnesota has taken steps to address the alleged fraud, including terminating its Housing Stabilization Services program, auditing autism services providers, adding new licensure requirements for autism centers, and pausing admissions of new providers into 13 high-risk Medicaid services. The state is also enhancing its review of claims using data analytics and artificial intelligence, increasing training for providers and employees, and increasing oversight of Medicaid managed care organizations.
Historically, CMS has addressed Medicaid fraud through claim disallowances and collaborative efforts with states to recoup funds. This new “compliance process,” however, allows the agency to withhold future payments based on a determination of “failure to comply substantially” with federal requirements – a shift that effectively penalizes states in anticipation of future fraudulent activity.
The Trump administration’s actions come as Medicaid faces renewed scrutiny regarding its long-term financial sustainability. House Budget Committee Chair Jodey Arrington (R-Texas) has stated that major changes to federal entitlement programs, including Medicaid, are necessary to address the national debt. The administration has also signaled an interest in revisiting policies related to Medicaid waivers, potentially encouraging states to adopt work requirements and other eligibility restrictions, as was the case during Trump’s first term.
A recent KFF analysis highlighted that Medicaid long-term care has shifted dramatically from institutional settings to home-based care. In 1981, home care accounted for just 1% of all long-term care spending; by 2023, it had risen to 64%. This shift reflects both consumer preferences and the impact of the 1999 Supreme Court ruling in Olmstead v. L.C., which affirmed the right of individuals with disabilities to receive care in the most integrated setting appropriate to their needs.
CMS released a new dataset on February 14, 2026, containing provider-level spending data intended to help identify unusual billing patterns. While the agency highlighted personal care as the top procedure in terms of spending, the data’s limitations – including the omission of institutional records and prescription drug costs – could lead to inaccurate conclusions, according to KFF.
Minnesota is appealing CMS’ decision and awaits a response to its revised corrective action plan.