Q&A: When Is It Safe to Skip Surgery for DCIS? – Medscape
The diagnosis of Ductal Carcinoma In Situ (DCIS) has long triggered an automatic reflex in oncology: immediate surgical excision. For decades, the medical consensus held that removing these abnormal cells was the only way to prevent progression to invasive breast cancer. However, emerging data from landmark clinical trials suggests a paradigm shift is underway. We are entering an era where “watchful waiting” may be as effective as the scalpel for specific low-risk patient profiles, challenging the historical standard of care and offering a reprieve from unnecessary surgical morbidity.
Key Clinical Takeaways:
- The COMET trial indicates that active surveillance for low-risk DCIS results in invasive cancer rates comparable to surgery over a 10-year period.
- Endocrine therapy remains a critical component of the non-surgical management protocol to suppress recurrence.
- Patient selection is rigorous; this approach is currently reserved for low-grade, hormone-receptor-positive cases, not high-grade pathology.
The Biological Rationale for De-Escalation
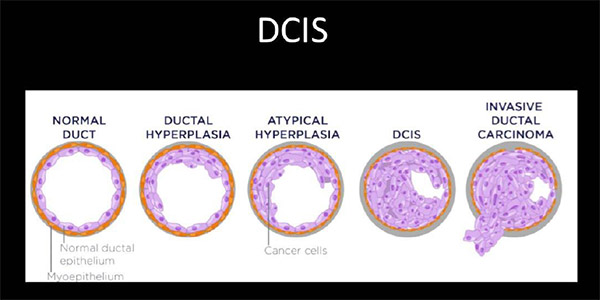
DCIS represents a proliferation of malignant cells confined within the milk ducts, lacking the ability to metastasize to distant organs. Historically, the fear driving surgical intervention was the statistical probability that these cells would breach the basement membrane and become invasive. Yet, autopsy studies and longitudinal data reveal that many women live with undiagnosed, indolent DCIS without ever developing symptoms. The clinical gap here is overtreatment. By subjecting all DCIS patients to lumpectomies or mastectomies, we expose them to surgical risks, anesthesia complications and psychological trauma for a condition that may never threaten their lives.
This realization has driven the design of the Comparison of Operative to Monitoring and Endocrine Therapy (COMET) trial. Funded by the National Cancer Institute (NCI) and the Department of Defense, this multi-institutional study sought to answer a question that has plagued breast surgeons for years: Is the risk of progression low enough to justify monitoring rather than cutting?
Deconstructing the COMET Trial Data
The COMET trial is a randomized, phase III study comparing standard surgical treatment against active surveillance combined with endocrine therapy. The study enrolled over 1,200 women with low-risk DCIS. The primary endpoint was the incidence of invasive breast cancer within the same breast over a ten-year follow-up period.
Early results, presented at major oncology conferences and peer-reviewed in journals such as JAMA Oncology, have been described as “reassuring” by lead investigators. The data suggests that for women with low-grade, hormone receptor-positive DCIS, the rate of invasive recurrence in the surveillance arm is statistically non-inferior to the surgery arm. This does not mean the cancer disappears; rather, it implies that the biological aggression of low-risk DCIS is slow enough that monitoring allows for timely intervention if progression occurs, without compromising survival outcomes.
| Clinical Parameter | Standard Surgical Care | Active Surveillance (COMET Protocol) |
|---|---|---|
| Primary Intervention | Lumpectomy or Mastectomy | Regular Imaging (Mammography/MRI) + Clinical Exam |
| Adjunct Therapy | Radiation (often) + Endocrine Therapy | Endocrine Therapy (Tamoxifen/Aromatase Inhibitors) |
| Invasive Recurrence Risk (10-Year) | Approx. 3-5% | Approx. 3-5% (Statistically Comparable) |
| Morbidity Profile | Surgical complications, scarring, recovery time | Psychological anxiety, medication side effects |
Clinical Triage and Patient Selection
It is vital to clarify that this “skip surgery” approach is not a blanket recommendation for all breast abnormalities. The eligibility criteria are stringent. Patients must have low-grade (Grade 1) DCIS that is estrogen-receptor positive. High-grade DCIS, which carries a significantly higher risk of rapid progression to invasive disease, remains a clear indication for surgical excision.
For patients navigating this complex decision matrix, the role of the specialist is paramount. Interpreting pathology reports to distinguish between low-risk and high-risk features requires subspecialty expertise. Patients facing a DCIS diagnosis should consider seeking a second opinion from board-certified breast surgeons who specialize in oncoplastic techniques and risk stratification. These specialists can determine if a patient’s specific genomic profile and imaging characteristics align with the COMET trial inclusion criteria.
“We are moving away from a ‘one-size-fits-all’ surgical mandate. The biology of low-risk DCIS suggests that for many women, the toxicity of surgery outweighs the benefit. Active surveillance allows us to treat the patient, not just the pathology report.”
This sentiment reflects the evolving consensus among leaders in breast oncology, including Dr. E. Shelley Hwang, the principal investigator of the COMET trial. Her work underscores that medical management is becoming a viable competitor to surgical management, provided the patient is compliant with rigorous monitoring schedules.
The Infrastructure of Active Surveillance
Choosing active surveillance over surgery shifts the burden of care from the operating room to the imaging suite. The success of this protocol relies entirely on high-fidelity diagnostic monitoring. If a lesion progresses, it must be detected immediately. This necessitates a robust relationship with diagnostic imaging centers capable of high-resolution mammography and potentially breast MRI.

endocrine therapy becomes the primary pharmacological defense. Medications like tamoxifen or aromatase inhibitors are used to block estrogen receptors, starving the DCIS cells of the fuel they need to grow. Managing the side effects of these drugs—ranging from hot flashes to bone density loss—requires a coordinated care team. Patients may benefit from consulting with medical oncologists who can tailor hormone suppression regimens to minimize quality-of-life impacts while maintaining efficacy.
The shift toward de-escalation likewise highlights the importance of genetic counseling. While DCIS is often sporadic, understanding a patient’s germline genetics (e.g., BRCA1/2 status) is essential before opting out of surgery. A patient with a known genetic mutation may still be advised to undergo prophylactic surgery despite low-risk DCIS findings. Integrating certified genetic counselors into the care plan ensures that the decision to skip surgery is based on a comprehensive understanding of the patient’s total risk profile.
Future Trajectory and Standard of Care
As we move through 2026, the integration of active surveillance into the National Comprehensive Cancer Network (NCCN) guidelines is accelerating. The data from the COMET trial provides the evidentiary backbone needed to change insurance coverage and clinical protocols. However, the transition requires patience. Changing decades of surgical dogma takes time, and not all providers are equally comfortable with non-operative management.
The future of DCIS treatment lies in precision medicine. We are moving toward a model where molecular profiling dictates the therapy, rather than the mere presence of abnormal cells. For now, the message is one of cautious optimism: surgery is no longer the only path forward for low-risk DCIS, but it remains the gold standard for high-risk disease. Patients must engage in shared decision-making, weighing the statistical safety of surveillance against the psychological comfort of excision.
For those considering this path, the first step is a rigorous review of your pathology and imaging by a multidisciplinary team. Ensure your care plan is built on the latest evidence by connecting with accredited cancer centers that participate in clinical research and adhere to the latest NCCN guidelines.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.