Medicare Part D: 2026 Enrollment, Premiums, and Cost Sharing Trends
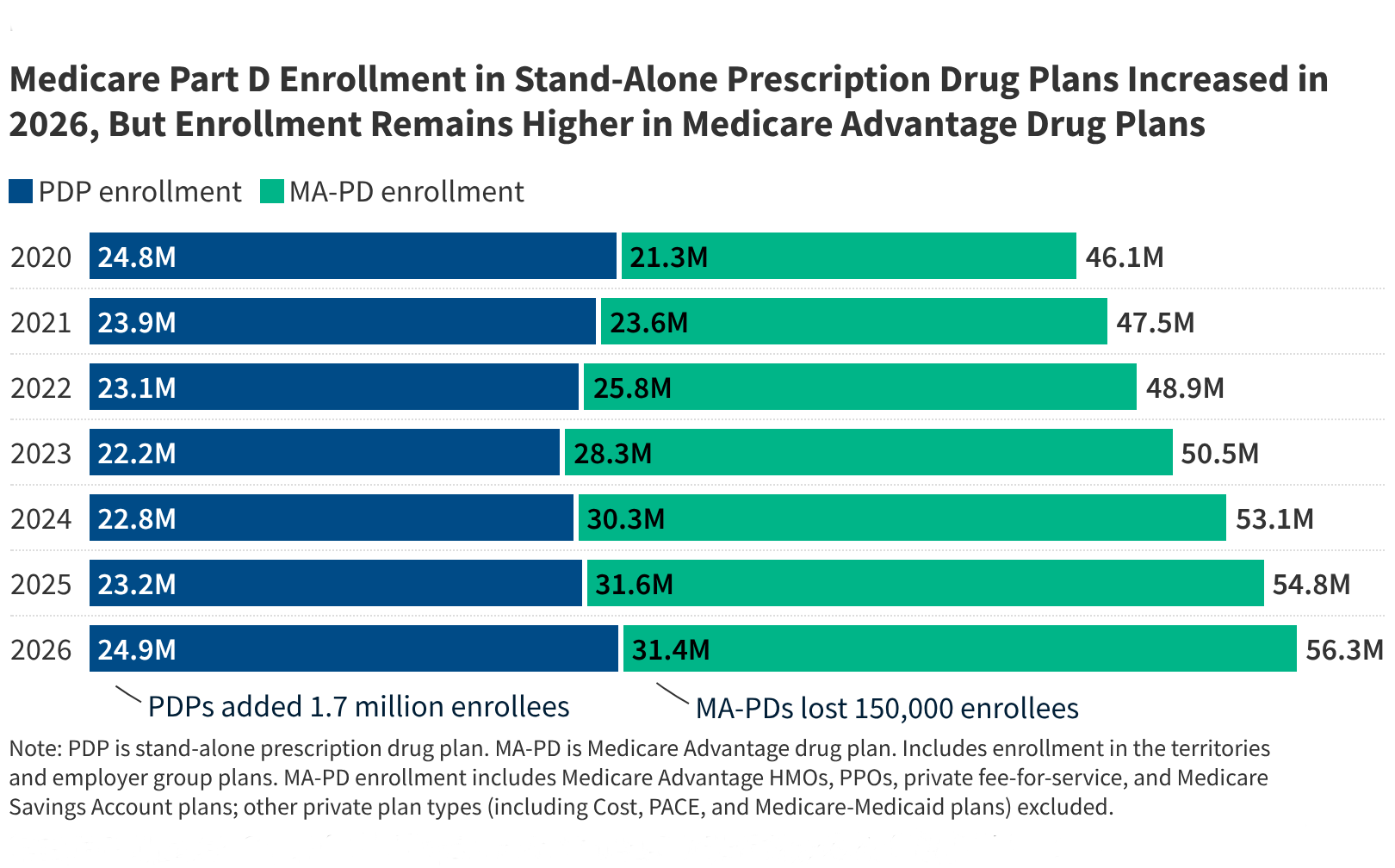
As of June 2026, the Centers for Medicare & Medicaid Services (CMS) reports that the Medicare Part D landscape serves 56 million beneficiaries, with significant shifts in cost-sharing structures and premium volatility driven by the implementation of the Inflation Reduction Act’s out-of-pocket spending caps. These adjustments fundamentally alter the financial threshold for patients requiring high-cost specialty pharmaceuticals, mandating a reassessment of coverage selection strategies for individuals managing chronic, multi-system pathologies.
Key Clinical Takeaways:
- Beneficiaries now benefit from a $2,000 annual cap on out-of-pocket prescription drug costs, significantly reducing the financial burden for those on high-cost maintenance therapies.
- Plan selection requires granular analysis of formulary tiers, as premium fluctuations are increasingly tied to the actuarial risk of specific patient cohorts.
- Clinical stability depends on proactive medication reconciliation and coordination with providers to ensure therapeutic continuity within evolving plan networks.
The Mechanism of Financial Risk in 2026 Medicare Part D
The current Medicare Part D framework has transitioned from a traditional “donut hole” model to a simplified structure centered on the $2,000 out-of-pocket maximum. According to CMS data, this shift aims to mitigate the morbidity associated with medication non-adherence, which often results from prohibitive cost-sharing requirements. When patients face high co-insurance for specialty biologics, the risk of therapeutic discontinuation increases, potentially exacerbating the underlying pathogenesis of conditions like rheumatoid arthritis, multiple sclerosis, or oncology-related comorbidities.

Dr. Elena Vance, a clinical pharmacologist and healthcare policy analyst, notes that “the transition to a hard cap on spending is a milestone for patient safety, yet it creates a secondary challenge where plans may aggressively manage utilization through stricter prior authorization and step-therapy protocols.” For patients requiring complex pharmacotherapy, this necessitates a partnership with specialized patient advocacy and pharmacy benefit consultants who can navigate the nuances of plan-specific formularies.
Epidemiological Impact and Therapeutic Continuity
The financial structure of Part D directly influences the standard of care for aging populations. Research published in JAMA underscores that out-of-pocket costs remain the primary driver of primary non-adherence among Medicare beneficiaries. In 2026, the legislative mandate for manufacturers to provide discounts in the initial coverage phase has forced a recalibration of plan premiums. While the $2,000 cap protects the individual, the administrative burden of ensuring that expensive specialty drugs remain covered under a chosen plan’s formulary has intensified.
Clinical stability is not merely a matter of drug efficacy but of consistent access. When a patient is forced to switch medications due to formulary changes—a process often dictated by the “least costly alternative” clinical guidelines—the risk of adverse events or loss of disease control rises. Patients experiencing difficulty with these transitions should consult with board-certified geriatricians or chronic disease specialists who are adept at documenting medical necessity for formulary exceptions.
Navigating Regulatory Hurdles and Supply Chain Stability
The 2026 enrollment cycle highlights a critical gap between insurance benefit design and the realities of modern clinical practice. Pharmaceutical distributors and pharmacy benefit managers (PBMs) are currently operating under heightened scrutiny regarding their rebate structures, which are funded in part by the Department of Health and Human Services (HHS) mandates. This regulatory environment creates a complex ecosystem where the cost of a drug is increasingly decoupled from its clinical utility, shifting the burden of cost management onto the beneficiary and their care team.

For healthcare institutions and private practices, this complexity demands rigorous compliance oversight. “Clinicians must ensure that their documentation of clinical necessity is ironclad, as the threshold for insurance approval for high-cost agents has never been higher,” states Dr. Marcus Thorne, an epidemiologist focusing on health systems. Practices and pharmacies seeking to maintain operational efficiency while supporting patient access often retain specialized healthcare compliance attorneys to manage the evolving regulatory landscape.
Future Trajectories in Medicare Benefit Design
Looking ahead, the focus of Medicare Part D will likely shift toward value-based pricing models, where reimbursement is tied to clinical outcomes rather than volume. As the current data suggests, the stabilization of the $2,000 cap is only the first step in a broader effort to rationalize the cost of pharmaceutical interventions for chronic illnesses. The success of these programs depends on the ability of both patients and providers to engage with the system proactively, utilizing data-driven insights to select plans that align with specific therapeutic needs.
As the 2027 enrollment period approaches, stakeholders must continue to monitor the intersection of clinical research and insurance policy. Understanding the nuances of these changes is essential for maintaining the standard of care in a shifting economic environment. For those seeking expert guidance on managing prescription costs alongside complex treatment plans, connecting with vetted medical billing and insurance navigation services remains a critical strategy for ensuring both clinical and financial health.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.