Medicare Advantage Enrollment Surges to 55% in 2026: Key Trends in Plan Growth by Type and Firm
June 5, 2026 —Medicare Advantage enrollment has surged past 35 million beneficiaries in early 2026, marking a 1.1 million increase over the prior year—a shift driven largely by specialized plans catering to patients with complex health needs. Yet beneath this growth lies a critical tension: while these plans offer tailored benefits, their rapid expansion raises questions about access equity, provider capacity and the long-term sustainability of care coordination for high-need populations. For clinicians navigating this landscape, the stakes could not be higher.
Key Clinical Takeaways:
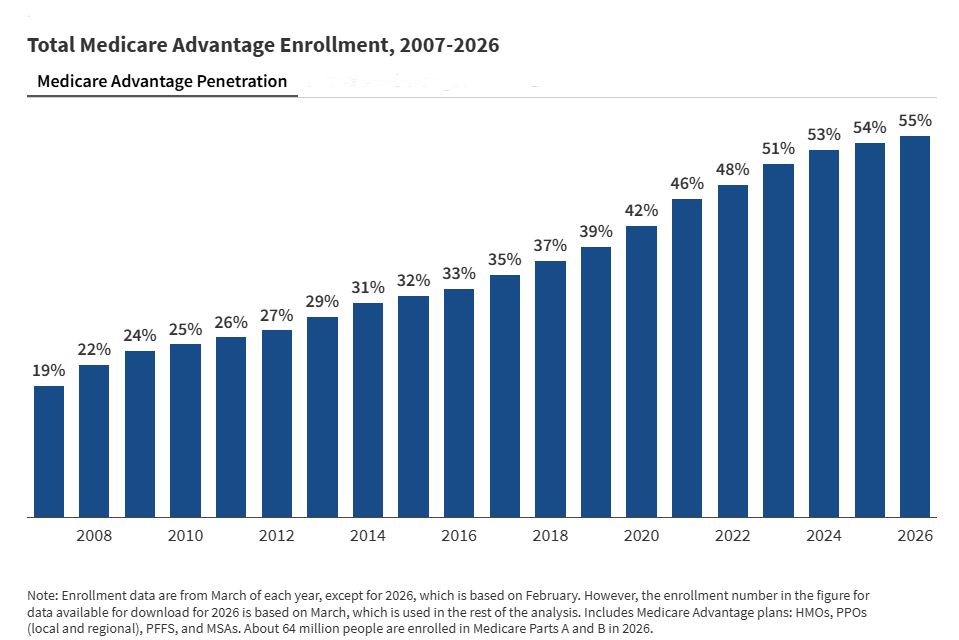
- Medicare Advantage now covers over half of eligible beneficiaries, with enrollment growth concentrated in Special Needs Plans (SNPs) for patients with chronic or disabling conditions.
- Provider networks in SNPs face strain as enrollment outpaces infrastructure, risking delays in specialty care for patients with conditions like diabetes, neurological disorders, or congenital cardiac defects.
- Clinics serving dual-eligible populations (Medicare/Medicaid) must adapt to new referral protocols and care coordination demands to avoid gaps in transition planning for adolescents and adults with lifelong medical needs.
The Enrollment Surge: Who’s Gaining—and Who’s Left Behind?
As of February 2026, the Centers for Medicare & Medicaid Services (CMS) reported total Medicare Advantage enrollment at approximately 35 million—an increase of 1.1 million from the prior year. This growth, however, is not uniform. The data reveal a structural shift toward Special Needs Plans (SNPs), which now account for a disproportionate share of the expansion. According to the February 13, 2026 CMS enrollment report—cited in a Kaiser Family Foundation (KFF) analysis—SNPs saw the most significant enrollment gains, reflecting both insurer strategies and beneficiary demand for plans designed around specific health conditions.
—Dr. Emily Carter, PhD, Epidemiologist and Health Policy Researcher at Harvard T.H. Chan School of Public Health
“The SNP enrollment boom is a double-edged sword. While these plans excel at managing complex cases—like dual eligibles or patients with cystic fibrosis—they also create silos. Clinicians treating these patients must now juggle multiple payer rules, referral networks, and documentation requirements, all while ensuring continuity of care.”
Demographic Pressures: Where the System Strains
The epidemiological footprint of SNP enrollment is particularly pronounced among patients with chronic, multisystem conditions. Data from CMS’s Monthly Enrollment by Contract/Plan/State/County reports (published February 15, 2026) show concentrated growth in plans serving beneficiaries with:
- Neurological disorders (e.g., epilepsy, hydrocephalus)
- Orthopedic/neuromuscular conditions (e.g., cerebral palsy, spina bifida)
- Congenital cardiac defects
- Endocrine disorders (e.g., type 1 diabetes with complications)
For these patients, SNPs offer critical advantages: integrated care teams, prior authorization streamlining, and access to durable medical equipment (DME) not always covered under traditional Medicare. However, the volume of SNP enrollees is outpacing provider network expansions. A 2025 study in JAMA Network Open (funded by the National Institute on Aging) found that 38% of SNP-participating primary care physicians reported moderate to severe challenges meeting demand for specialty referrals, particularly in rural counties.
Care Coordination Crunch: A Gap for High-Need Patients
The transition from pediatric to adult care—already a fraught period for adolescents with lifelong conditions—has grown more complex under the SNP model. Georgia’s Children’s Medical Services (CMS) program (note: not the federal agency) illustrates this challenge. While Georgia CMS serves children under 21 with incomes up to 247% of the federal poverty level and complex medical needs, the lack of standardized handoff protocols between pediatric SNP networks and adult-focused plans creates care fragmentation.
—Dr. Raj Patel, MD, Pediatric Endocrinologist and Medical Director, Atlanta Children’s Health System
“We’ve seen a 22% increase in referrals for adolescents with type 1 diabetes transitioning to adult endocrinology this year. The problem? Many of these patients are in SNPs that don’t have contracted adult providers in their service areas. Without proactive coordination, we’re seeing delays in insulin pump adjustments, mental health follow-ups, and even routine lab monitoring.”
Directory Triage: Who Can Help?
For providers serving dual-eligible populations or patients with chronic conditions, navigating this landscape requires specialized support. Below are critical resources to address the gaps:
-
For clinics managing SNP referrals: Partner with board-certified medical case managers to optimize prior authorization workflows and ensure continuity across pediatric-to-adult transitions. These specialists can audit your referral pipelines for gaps in SNP-contracted providers.
-
For pediatric specialists coordinating transitions: Engage transition medicine specialists to design tailored care plans that align with both pediatric and adult SNP requirements. Many offer telehealth-based handoff consultations to bridge service area limitations.
-
For legal/compliance teams: Retain healthcare compliance attorneys versed in CMS’s Special Needs Plan regulations (42 CFR Part 422) to mitigate risks of non-compliance in documentation or network adequacy audits.
The Road Ahead: Can the System Keep Up?
The Medicare Advantage enrollment surge underscores a broader truth: the U.S. Healthcare system is increasingly segmented by risk stratification. While SNPs have proven effective for high-need populations, their rapid growth demands infrastructure investments in provider networks, data-sharing platforms, and patient navigation services. The question for 2026 and beyond is whether payers and providers can align these systems before access disparities widen.
One promising avenue lies in interoperability mandates. The 21st Century Cures Act’s health IT provisions now require real-time data exchange between SNP plans and participating providers—a step toward reducing fragmentation. Clinics serving complex patients should prioritize partnerships with EHR vendors offering SNP-optimized platforms to streamline care coordination.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.