Genetic Testing and Polygenic Risk Scores for Cardiovascular Disease Prediction
The paradigm of cardiovascular risk assessment is shifting from reactive management to genomic anticipation. For decades, clinicians have relied on a handful of phenotypic markers to predict heart disease, but a latest frontier in polygenic risk scoring is revealing a hidden layer of vulnerability that traditional calculators consistently overlook.
Key Clinical Takeaways:
- Polygenic Risk Scores (PRS) identify hereditary predispositions for up to eight distinct cardiovascular pathologies, offering a more granular risk profile than standard metrics.
- Genetic screening can predict a risk of coronary heart disease that is up to 3.7 times higher than what is indicated by traditional clinical markers.
- PRS does not replace traditional risk scores but complements them, allowing for aggressive early intervention in patients who otherwise appear “low risk.”
Traditional cardiovascular risk models—such as the Framingham Risk Score or the ASCVD Risk Estimator—rely heavily on established biomarkers: blood pressure, LDL cholesterol levels, age, and smoking status. While these tools are essential for population health, they operate on a “snapshot” logic, measuring the current state of the patient’s physiology. The clinical gap lies in the “silent” genetic burden—the cumulative effect of thousands of minor genetic variations that dictate how a patient’s body handles inflammation, lipid metabolism, and arterial integrity long before a blood pressure cuff registers a problem.
The Biological Architecture of Polygenic Risk
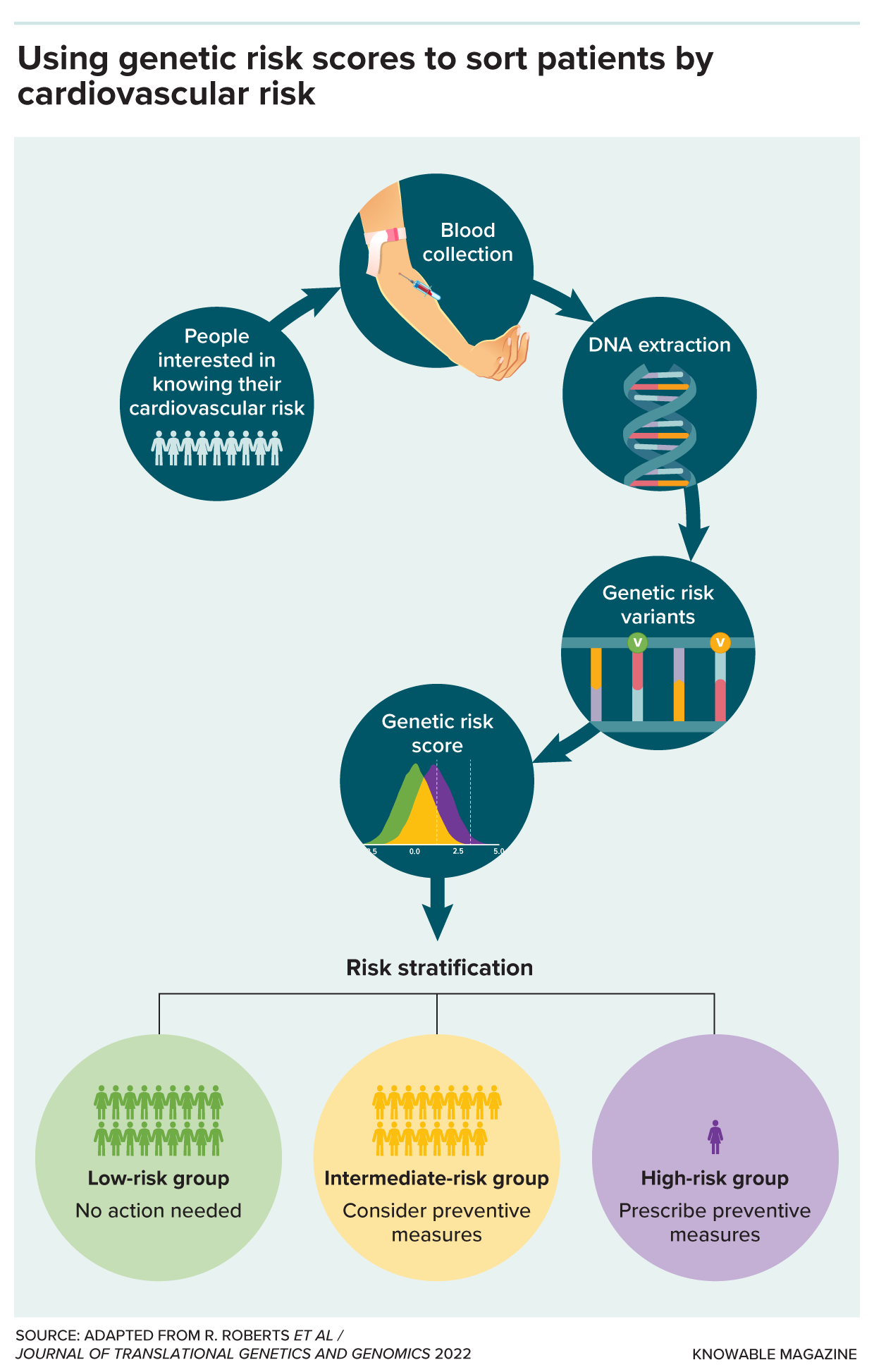
Unlike monogenic disorders, where a single mutation (such as in familial hypercholesterolemia) causes a disease, most cardiovascular conditions are polygenic. They result from the additive effect of numerous Single Nucleotide Polymorphisms (SNPs) across the genome. A Polygenic Risk Score (PRS) aggregates these thousands of tiny variations into a single numerical value, representing a patient’s genetic liability relative to the general population.

This genomic mapping focuses on the complex interplay between inflammation, genetics, and metabolism. By analyzing these markers, clinicians can identify individuals with a high genetic predisposition who may have “normal” cholesterol levels but possess an underlying pathogenesis that accelerates plaque buildup. For patients exhibiting these high-risk genomic signatures, the standard of care is evolving toward earlier and more aggressive preventative therapies.
To properly interpret these complex genomic results, patients should not rely on direct-to-consumer kits. We see imperative to consult with certified genetic counselors who can translate raw SNP data into clinical action plans, ensuring that the psychological impact of a high-risk score is managed alongside the medical intervention.
Clinical Comparison: Traditional vs. Polygenic Assessment
The integration of PRS into clinical workflows creates a dual-layered defense. While traditional scores advise us where a patient is now, the PRS tells us where they are headed. The following table outlines the divergence in these two diagnostic approaches:
| Feature | Traditional Risk Scores (e.g., ASCVD) | Polygenic Risk Scores (PRS) |
|---|---|---|
| Data Source | Phenotypic (BP, Cholesterol, Age, BMI) | Genotypic (Genome-wide SNP analysis) |
| Temporal Nature | Dynamic (Changes with lifestyle/age) | Static (Fixed from birth) |
| Predictive Focus | Short-to-medium term event probability | Lifetime hereditary susceptibility |
| Clinical Utility | Determines current medication needs | Determines timing and intensity of screening |
| Sensitivity | May miss “healthy” high-risk patients | Identifies risk regardless of current biomarkers |
Translating Genomic Data into Preventative Cardiology
The ability to predict a 3.7-fold increase in coronary heart disease risk transforms the clinical timeline. When a patient is identified as high-risk via PRS, the window for primary prevention opens years, or even decades, earlier. This allows for the implementation of precision medicine—tailoring statin therapy or antihypertensive regimens based on the patient’s specific metabolic and genetic map.
This shift requires a multidisciplinary approach. The identification of high polygenic risk often necessitates a referral to board-certified cardiologists who specialize in preventative cardiology. These specialists can utilize advanced imaging, such as Coronary Artery Calcium (CAC) scoring, to see if the genetic risk has already begun to manifest as physical arterial calcification.

“The integration of genomic risk scores allows us to move beyond the ‘average patient’ model. We can now identify the outliers—those whose genetics place them at extreme risk despite a healthy lifestyle—and provide them with a level of surveillance that was previously reserved for those already symptomatic.”
The development of these tests often stems from large-scale Genome-Wide Association Studies (GWAS), which analyze the DNA of hundreds of thousands of individuals to correlate specific SNPs with cardiovascular events. These studies, frequently funded by national health institutes and university research consortures, provide the statistical power necessary to validate PRS as a reliable clinical tool. For those seeking the most advanced screening, utilizing specialized diagnostic centers equipped for high-throughput genomic sequencing is the current gold standard.
The Future of Cardiovascular Triage
As we refine the “map” of cardiovascular risk, the focus is shifting toward the synergy between genetics and epigenetics. While the PRS provides the blueprint, lifestyle factors—diet, exercise, and stress management—act as the switches that turn these genes on or off. The ultimate goal of precision cardiology is to determine exactly which lifestyle interventions are most effective for specific genetic profiles, effectively “silencing” high-risk alleles through targeted behavior.
The transition toward genomic-informed care is not without hurdles, particularly regarding data privacy and the potential for insurance discrimination. However, the clinical benefit of preventing a myocardial infarction through early detection far outweighs the systemic challenges. By bridging the gap between genomic data and clinical practice, the medical community is moving toward a future where heart disease is not just managed, but preempted.
For those with a significant family history of heart disease, waiting for traditional biomarkers to shift may be a dangerous strategy. Proactive genomic screening, paired with a vetted team of specialists, represents the most robust defense available in modern medicine.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.