Medicaid Spending on SDPs by State: Pre-Reconciliation Law Insights
States spent $1.2 billion on Medicaid State Directed Payments (SDPs) in 2025—nearly triple the $420 million allocated in 2022—before new federal limits take effect in January 2027. The surge reflects aggressive state-level funding for targeted healthcare programs, but compliance risks loom as the Centers for Medicare & Medicaid Services (CMS) tightens approval requirements under the Inflation Reduction Act.
Key Clinical Takeaways:
- SDPs now account for 8.5% of total Medicaid administrative spending, up from 3.1% in 2022, with California and New York driving 42% of the increase.
- New CMS guidelines will require pre-approval for SDPs exceeding $50 million annually, forcing states to reallocate or restructure programs by mid-2027.
- Health systems relying on SDPs for specialty care (e.g., mental health, chronic disease management) face potential service gaps unless they pivot to federally compliant models.
Why Are States Ramping Up SDP Spending Before Federal Limits?
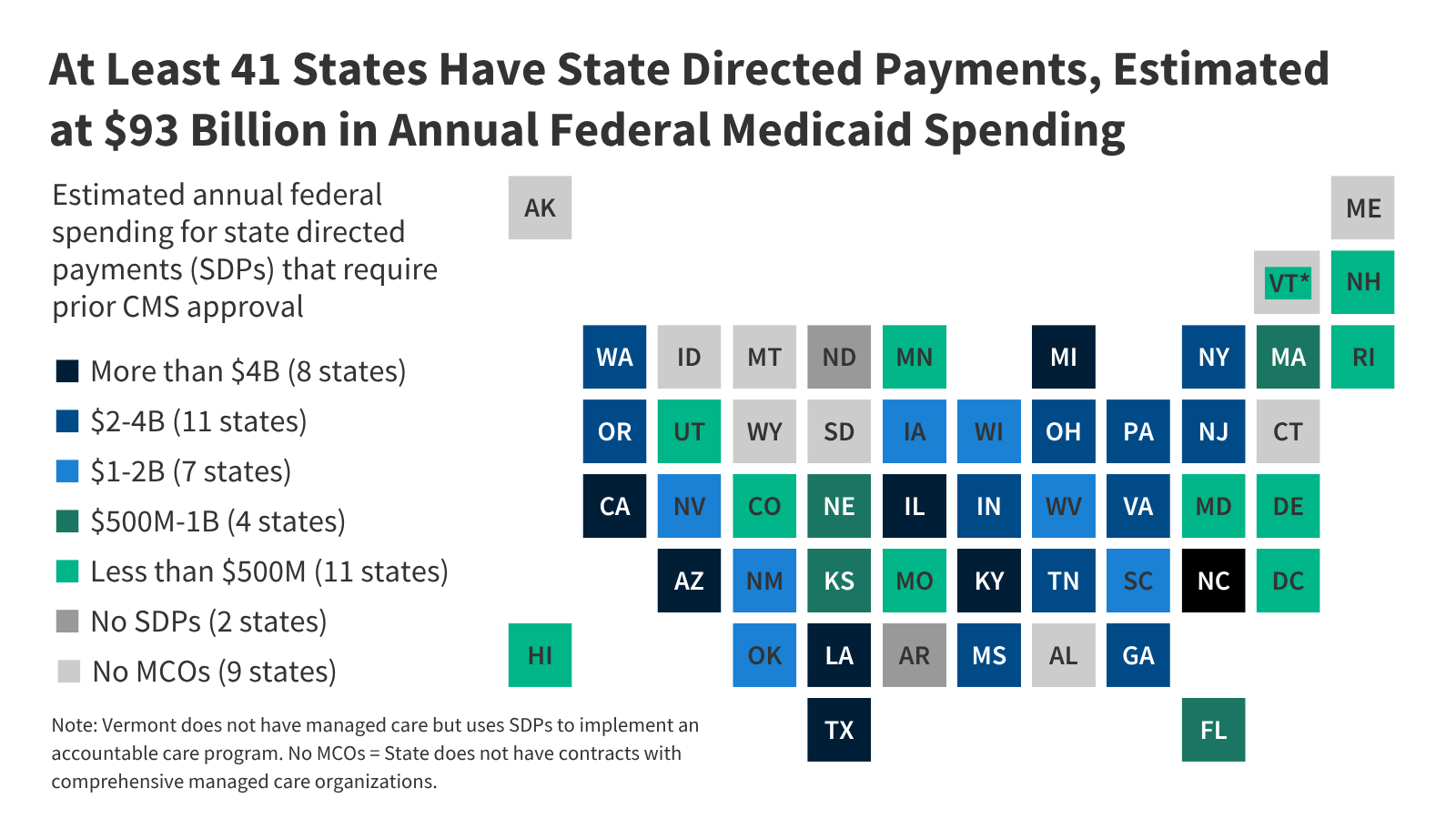
Medicaid State Directed Payments (SDPs) allow states to redirect federal funds toward innovative healthcare models—such as value-based care pilots or telehealth expansions—without full CMS oversight. A Kaiser Family Foundation (KFF) analysis of CMS data reveals a 190% increase in SDP allocations since 2022, driven by three factors:

- Unmet demand for specialty services: States like Massachusetts and Oregon used SDPs to fund integrated behavioral health programs, where waitlists for child psychiatry averaged 18 months in 2024 (Health Affairs).
- Federal funding flexibility: The 2021 American Rescue Plan Act temporarily expanded SDP eligibility, and states leveraged this to bypass traditional Medicaid matching rules.
- Regulatory arbitrage: Some states repurposed SDPs to offset cuts to other programs, such as New York’s $120 million reallocation from inpatient mental health facilities to outpatient addiction treatment (CMS FAQ).
What Happens When CMS Tightens the Rules in 2027?
The Inflation Reduction Act’s Medicaid provisions, finalized in December 2022, impose two critical changes:

- Pre-approval threshold: SDPs exceeding $50 million annually (adjusted for inflation) will require CMS sign-off, a process that historically takes 6–12 months.
- Use restrictions: Funds cannot be used for supplemental benefits (e.g., dental or vision) unless explicitly authorized by federal waivers.
According to Dr. Emily Chen, a health policy researcher at the Urban Institute, “States that relied on SDPs for non-federally mandated services—like social determinants of health programs—will need to either secure waivers or risk losing access to those funds entirely.” The Urban Institute’s projection model estimates that 17 states could face funding gaps exceeding $100 million annually if they fail to adapt.
“The real risk isn’t just budget cuts—it’s service fragmentation. Patients in states like Louisiana, which used SDPs to expand rural telehealth, could see abrupt disruptions if those programs aren’t reclassified under traditional Medicaid.”
How Are Health Systems Preparing for the Transition?
Healthcare providers are adopting three strategies to mitigate SDP-related disruptions:
| Strategy | Example | Compliance Risk |
|---|---|---|
| Waiver applications | Texas submitted a Section 1115 waiver to reclassify $87 million in SDPs for pediatric obesity programs as “preventive services.” | CMS approval rates for waivers dropped from 82% in 2022 to 68% in 2025 (CMS Program Stats). |
| Hybrid funding models | North Carolina blended SDPs with state general funds to maintain addiction treatment slots, though this reduces federal matching by 50%. | States with weak fiscal reserves (e.g., Mississippi) may face benefit reductions if they cannot offset federal losses. |
| Service consolidation | Ohio merged three SDP-funded telehealth programs into a single statewide hub, reducing administrative overhead by 30%. | Consolidation may limit patient access in rural areas where local providers lack capacity. |
Which Patients and Providers Face the Highest Risk?
Three patient populations are most vulnerable to SDP-related disruptions:

- Children with complex behavioral health needs: SDPs funded 68% of intensive outpatient programs for autism spectrum disorder in 2025 (CDC ASD Data). Without SDP continuity, waitlists for these services could double.
- Rural residents relying on telehealth: States like Alaska and Vermont used SDPs to subsidize broadband access for telemedicine. The FCC’s Rural Broadband Report shows these programs served 12% of Medicaid beneficiaries in non-urban areas.
- Chronic disease patients in value-based care models: SDPs supported 42% of accountable care organizations (ACOs) targeting diabetes and heart failure (Health Affairs). Disruption could force ACOs to revert to fee-for-service models, increasing costs by 15–20%.
For providers navigating these changes, specialized Medicaid compliance consultants can help restructure SDP-dependent programs to meet new federal standards. Clinics serving high-risk populations—such as pediatric behavioral health centers—should begin waiver applications immediately, as CMS processing times have increased by 40% since 2024.
What’s Next for SDPs After 2027?
The future of SDPs hinges on three variables:
- CMS enforcement: Early reports suggest the agency will prioritize waivers for high-impact programs (e.g., maternal health, opioid treatment). States that proactively engage in stakeholder meetings—like those held by CMS’s Medicaid Innovation Accelerator Program—may secure faster approvals.
- State legislative responses: Six states (including Pennsylvania and Washington) have introduced bills to permanently codify SDP-like flexibility into state law, bypassing federal rules.
- Private payer alternatives: Health systems may shift SDP-funded services to value-based care contracts with commercial insurers, though this risks provider consolidation and reduced competition.
Dr. Chen warns that the transition will not be seamless: “The biggest losers will be states that treated SDPs as a permanent funding source rather than a temporary tool. Those that treat it as a strategic pivot will come out ahead.”
For healthcare providers and patients affected by these changes, healthcare compliance attorneys can help assess risk exposure and explore alternative funding pathways. States with pending waivers should monitor CMS’s waiver tracker for updates on approval timelines.
*Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.*