
Medicaid Waiver Tracker Reveals Shifting Landscape of Coverage for Incarcerated Individuals and Children
Table of Contents
As of September 23, 2024, a new wave of state-level Medicaid waivers is reshaping access to healthcare for both incarcerated individuals preparing for release and children requiring continuous eligibility. Recent data from the Kaiser Family Foundation (KFF) highlights both expansions in pre-release coverage and impending changes to continuous eligibility programs,impacting millions of Medicaid beneficiaries nationwide. These shifts come amid ongoing debates about healthcare access,criminal justice reform,and the efficient governance of public health programs.
The KFF Medicaid Waiver Tracker and accompanying waiver watch (August 2024) detail a growing trend of states seeking waivers to provide Medicaid coverage to individuals prior to their release from incarceration. Simultaneously, the future of multi-year continuous eligibility for children is uncertain, as the Trump administration signaled a halt to new and extended waivers. This dual trajectory presents both opportunities and challenges for maintaining consistent healthcare access for vulnerable populations.
Pre-Release Medicaid Coverage Gains Momentum
States are increasingly utilizing Section 1115 waivers to initiate Medicaid coverage for incarcerated individuals in the months leading up to their release. This pre-release coverage aims to improve health outcomes, reduce recidivism, and facilitate a smoother transition back into the community. The KFF data shows a growing number of states implementing or seeking approval for these programs.

Did You Know?
Pre-release Medicaid coverage can help individuals address chronic health conditions, connect with behavioral health services, and establish a primary care provider before leaving incarceration, reducing the likelihood of emergency room visits and improving overall health stability.
Multi-year Continuous Eligibility for Children Faces Uncertainty
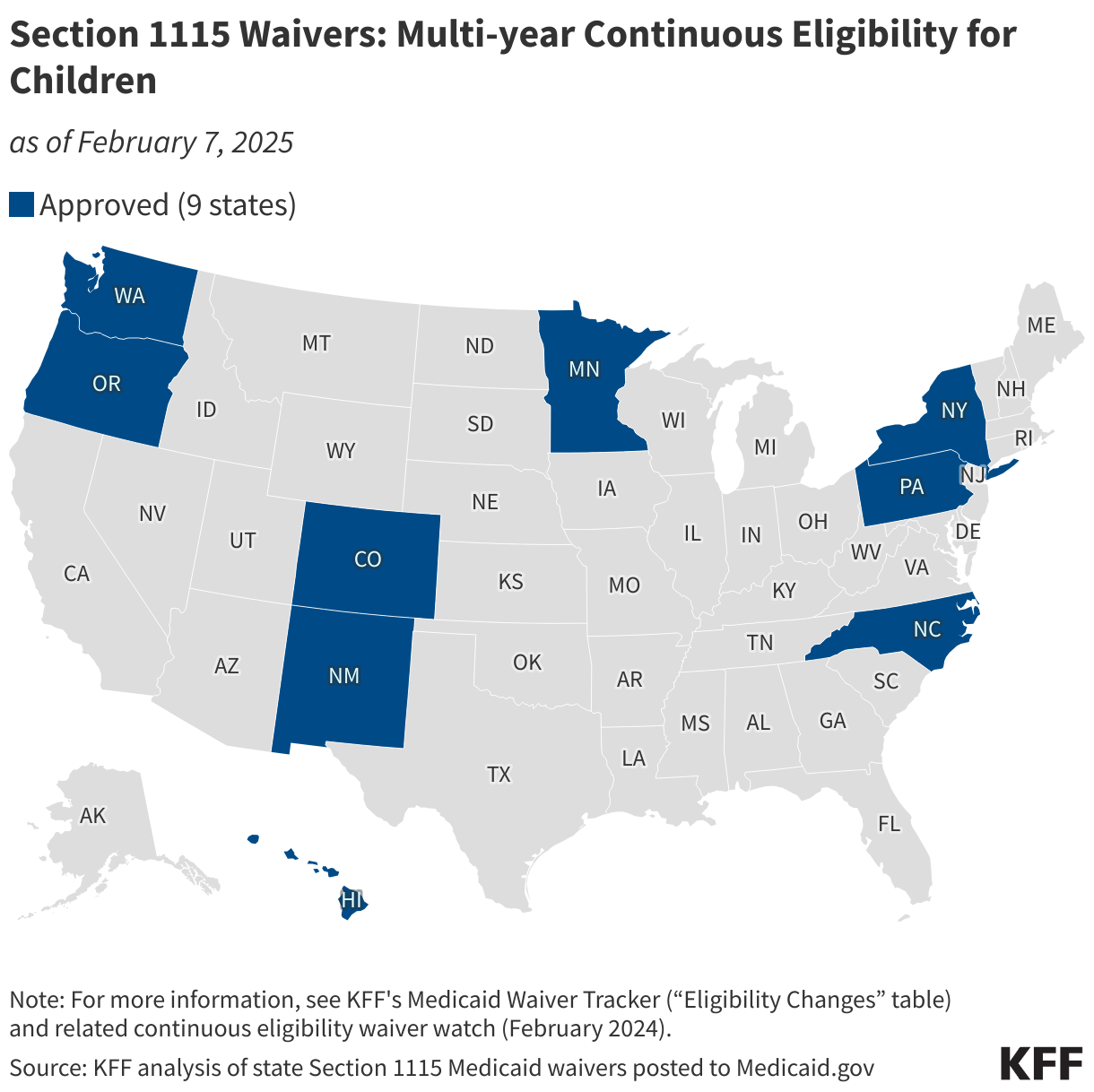
The Consolidated Appropriations Act,2023 mandated 12-month continuous eligibility for children,starting January 1,2024. Building on this, the Biden administration approved nine waivers allowing states to extend this to multi-year continuous eligibility, perhaps covering children from birth to age six. Research from the Medicaid and CHIP Payment and Access Commission (MACPAC) demonstrates that continuous eligibility reduces Medicaid disenrollment and “churn” – the frequent loss and re-enrollment in coverage.
However, in July 2025, guidance from the Trump administration indicated a shift in policy, stating it would not approve new or extend existing continuous eligibility waivers for children or adults. The map below illustrates states currently approved to provide multi-year continuous eligibility for children.
Pro Tip:
To stay informed about changes to Medicaid eligibility in your state, regularly consult the KFF Medicaid Waiver Tracker and sign up for KFF alerts.
| Waiver Type | focus | Key Dates | Impacted Population |
|---|---|---|---|
| Section 1115 | Pre-release Coverage | Ongoing (2024-2025) | Incarcerated Individuals |
| Section 1115 | Continuous Eligibility | Jan 1, 2024 – July 2025 | Children (0-6) |
| Consolidated Appropriations Act | 12-Month Continuous Eligibility | Jan 1, 2024 | All Children |
These developments underscore the dynamic nature of Medicaid policy and the importance of ongoing monitoring of waiver approvals and federal guidance.The future of healthcare access for both incarcerated individuals and children remains subject to political and administrative changes.
Section 1115 waivers allow states to test new approaches in Medicaid and CHIP that differ from statutory requirements.
What are your thoughts on the potential impact of ending continuous eligibility for children? How can states best utilize waivers to improve healthcare access for individuals re-entering society after incarceration?
Background: Medicaid Waivers and Section 1115
Medicaid waivers, authorized under Section 1115 of the Social Security Act, provide states with versatility to design and implement innovative programs that differ from standard Medicaid requirements.These waivers are subject to federal approval and are often used to address specific state needs, such as expanding coverage to new populations or testing option delivery systems. The use of waivers has become increasingly common in recent years, as states seek to address challenges related to healthcare access, cost containment, and quality improvement. The Consolidated Appropriations Act of 2023 built upon existing efforts to streamline eligibility and reduce administrative burdens for beneficiaries.
Frequently Asked Questions about Medicaid Waivers
- What is a Medicaid waiver? A Medicaid waiver is a permission granted by the federal government to a state allowing it to modify certain Medicaid rules to better serve its population.
- What is Section 1115 of the Social Security Act? Section 1115 is the part of the social Security act that allows states to request waivers to test new approaches in Medicaid.
- How do pre-release Medicaid waivers work? These waivers allow states to enroll incarcerated individuals in Medicaid before their release, providing them with healthcare services and support during their transition back into the community.
- What is continuous Medicaid eligibility? Continuous eligibility means that once someone is determined eligible for Medicaid, their coverage lasts for a specified period (e.g., 12 months or longer) without requiring periodic redetermination.
- What is the potential impact of ending continuous eligibility for children? Ending continuous eligibility could lead to increased churn, disenrollment, and gaps in coverage for children, potentially impacting their health and well-being.
- Where can I find more data about Medicaid waivers? The KFF Medicaid Waiver Tracker is an excellent resource.
If you found this information valuable, please share it with your network and join the conversation! Subscribe to our newsletter for the latest updates on Medicaid policy and healthcare access.