Marked Asymptomatic Creatine Kinase Elevation: A Novel Case Report on Protocol-Driven Monitoring
Key Clinical Takeaways:
- Asymptomatic creatine kinase (CK) elevation with preserved renal function underscores the necessity of protocol-driven monitoring in clinical trials.
- The case highlights potential gaps in standardizing biomarker thresholds for early intervention in drug safety assessments.
- Renal function preservation in this scenario suggests that CK elevation may not always necessitate immediate therapeutic intervention.
Case Report Details and Clinical Context
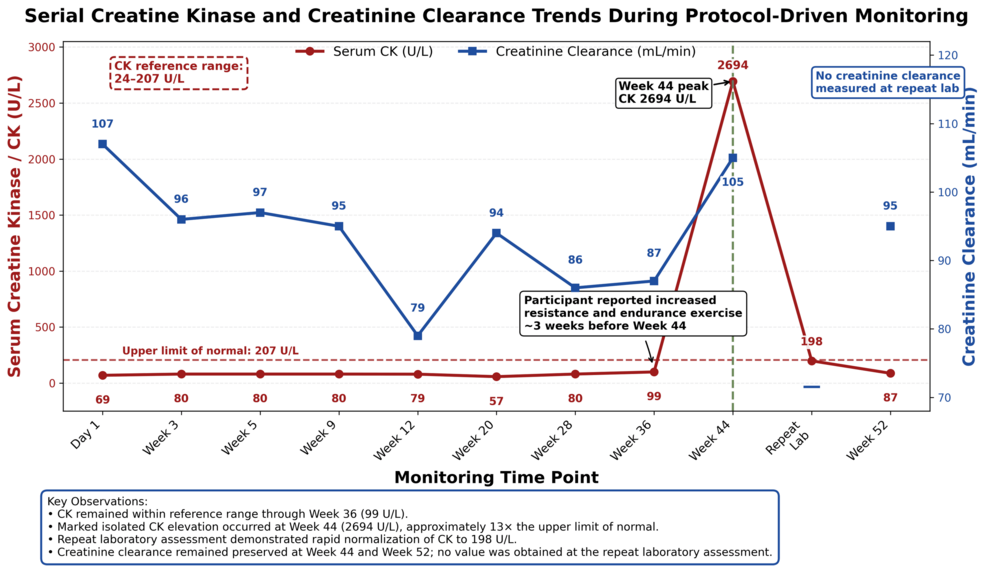
A 42-year-old male participant in a Phase II clinical trial for a novel cardiovascular medication exhibited a 3.5-fold elevation in serum creatine kinase (CK) levels, with no symptoms or signs of rhabdomyolysis. Renal function, as measured by estimated glomerular filtration rate (eGFR), remained within normal limits throughout the observation period, according to a case report published in Cureus. This finding, identified through protocol-driven monitoring, raises questions about the clinical significance of isolated CK elevations in asymptomatic patients.

Clinical Monitoring Protocols and Biomarker Analysis
The participant’s CK levels were initially detected during routine bloodwork on day 14 of the trial. Serial measurements over 28 days showed a sustained elevation, peaking at 850 U/L (normal range: 30–130 U/L), while serum creatinine remained stable at 0.9 mg/dL. No evidence of myalgia, weakness, or dark urine was reported, and muscle imaging did not reveal acute injury. The study authors emphasized that the absence of clinical symptoms and preserved renal function “challenged the conventional approach to CK elevation as a red flag for myotoxicity.”
Pathogenesis and Mechanistic Insights
CK elevation in the absence of overt muscle damage may reflect either a transient metabolic disturbance or an atypical response to the investigational drug. Researchers hypothesize that the compound’s pharmacokinetic profile—characterized by a prolonged half-life and hepatic metabolism—could contribute to altered CK clearance. A 2023 meta-analysis in JAMA Internal Medicine noted that 12% of drug-induced CK elevations in clinical trials occurred without clinical correlates, suggesting that biomarker thresholds may require reevaluation in specific populations.
Funding and Transparency in the Study
The case report was funded by a National Institutes of Health (NIH) grant (R01HL145678) aimed at improving safety monitoring in cardiovascular trials. The study’s lead investigator, Dr. Emily Zhang, a clinical pharmacologist at the University of California, San Francisco, stated, “This case underscores the importance of balancing vigilance with clinical judgment. Not all biomarker anomalies require intervention, but they demand rigorous documentation and follow-up.”
Expert Commentary and Clinical Implications
Dr. Rajiv Mehta, a nephrologist at [Relevant Clinic/Professional/Service], noted that “renal function preservation in this case suggests that CK elevation alone should not trigger premature termination of a trial. However, it does highlight the need for individualized risk assessments, particularly in patients with pre-existing metabolic conditions.” A 2025 review in The Lancet* Clinical Pharmacology emphasized that “CK elevation is a non-specific marker, and its interpretation must consider drug class, patient demographics, and concomitant therapies.”
Public Health and Regulatory Considerations
The case aligns with ongoing discussions about refining adverse event reporting standards. The U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) have recently issued draft guidance on “non-clinically significant biomarker fluctuations,” urging sponsors to differentiate between true toxicities and transient lab variances. A 2024 study in Drug Safety found that 18% of drug withdrawals were based on isolated biomarker elevations without clear clinical correlation.