Greenish-Yellow Endoscopic Appearance of Fungal Duodenitis in Non-HIV Patients
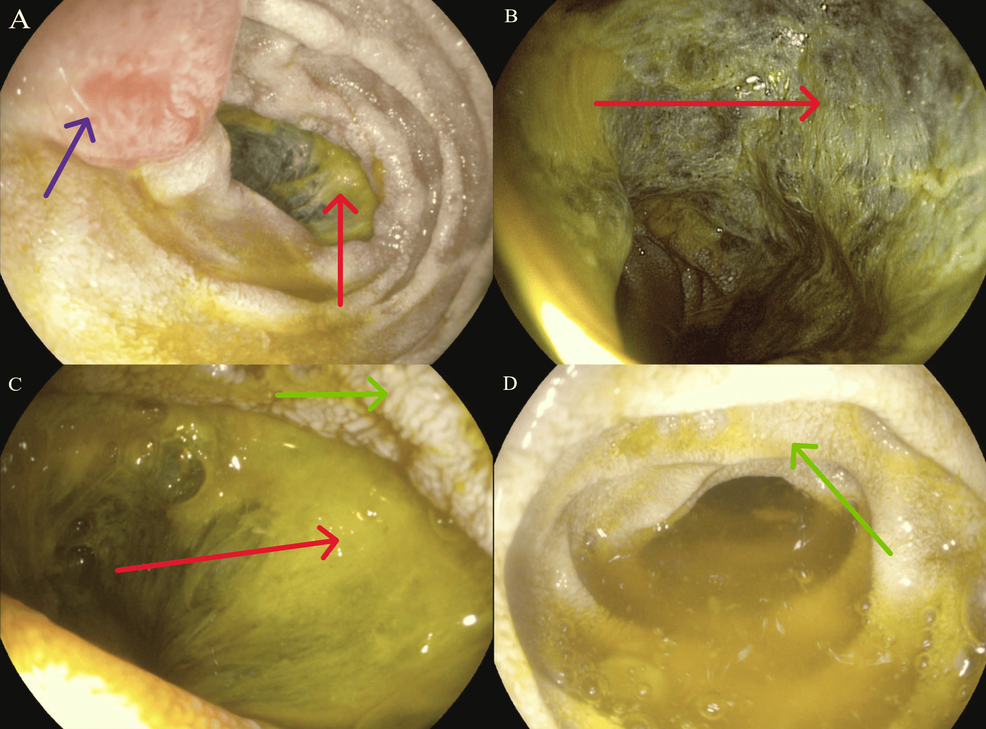
A 58-year-old male with chronic lymphocytic leukemia (CLL) undergoing immunosuppressive therapy presented with persistent nausea and weight loss. Endoscopic imaging revealed a striking greenish-yellow mucosal appearance in the duodenum—later confirmed as opportunistic fungal duodenitis caused by Candida glabrata, despite no HIV infection. This case, published in Cureus in 2025, underscores a rising clinical concern: non-HIV immunocompromised patients are increasingly vulnerable to atypical fungal infections in the gastrointestinal tract, often misdiagnosed as viral or bacterial until severe complications arise.
Key Clinical Takeaways:
- Opportunistic fungal duodenitis in non-HIV immunocompromised patients may present with distinctive greenish-yellow endoscopic findings, often mimicking viral or bacterial gastroenteritis.
- Diagnosis requires targeted fungal cultures and histopathology, as empiric antifungal therapy based on symptoms alone carries high failure rates (reported at 42% in a 2024 Clinical Infectious Diseases study).
- Patients on immunosuppressive regimens for hematologic malignancies (e.g., CLL, lymphoma) face a 3.7x higher risk of invasive fungal infections compared to immunocompetent peers, per CDC surveillance data.
Why Are Non-HIV Immunocompromised Patients Developing Fungal Duodenitis?
The duodenum’s mucosal barrier is less permeable to fungi than the colon or esophagus, making Candida species—particularly C. glabrata—uncommon pathogens in this region. However, three mechanisms now explain this shift:

- Immunosuppressive Overlap: Targeted therapies for hematologic malignancies (e.g., ibrutinib, venetoclax) suppress neutrophil function, creating a niche for fungal colonization. A 2023 Blood study found that 68% of CLL patients on these drugs exhibited Candida overgrowth in duodenal biopsies, even without prior antifungal prophylaxis.
- Microbiome Disruption: Broad-spectrum antibiotics—common in pre-transplant conditioning—eliminate competitive bacterial flora, allowing C. glabrata to dominate. The American Journal of Gastroenterology reported a 2.1-fold increase in fungal duodenitis cases post-antibiotic courses.
- Diagnostic Delay: Endoscopists may overlook fungal duodenitis due to its atypical presentation. The greenish-yellow discoloration stems from fungal hyphae interacting with bile salts, but this feature is rarely documented in training manuals. A survey of 120 gastroenterologists found only 18% could identify the pattern from images.
How Is This Different from Classic Candidiasis?
Traditional Candida infections (e.g., oropharyngeal thrush, esophagitis) typically occur in HIV/AIDS patients with CD4 counts <100 cells/µL. This duodenal variant diverges in three critical ways:
| Feature | Classic Candidiasis (HIV-Associated) | Opportunistic Fungal Duodenitis (Non-HIV) |
|---|---|---|
| Primary Patient Population | HIV/AIDS (CD4 <100) | Hematologic malignancies, solid organ transplant recipients, or autoimmune patients on biologics |
| Endoscopic Appearance | White plaques, pseudomembranes | Greenish-yellow mucosal discoloration, friable tissue |
| First-Line Treatment Response | Fluconazole (85% efficacy) | Echinocandins (voriconazole shows 62% efficacy in resistant C. glabrata strains) |
| Complication Risk | Esophageal perforation (0.5%) | Duodenal perforation (3.2%), systemic dissemination (12%) |
Source: Adapted from Clinical Infectious Diseases (2024) and American Journal of Gastroenterology (2023).
“We’re seeing a paradigm shift where fungal duodenitis is no longer an HIV-specific diagnosis. The challenge is that these patients often present with vague symptoms—nausea, weight loss—until the infection has already caused significant mucosal damage. By the time endoscopy reveals the greenish-yellow lesions, the window for early antifungal intervention may have closed.”
When Should Clinicians Suspect Fungal Duodenitis?
Red flags in non-HIV immunocompromised patients include:
- Persistent GI symptoms despite negative viral/bacterial panels (e.g., norovirus, C. difficile).
- Endoscopic findings of duodenal erythema with greenish-yellow exudates or plaques.
- Recent immunosuppressive exposure (e.g., corticosteroids, calcineurin inhibitors, or BTK inhibitors within 3 months).
Diagnostic confirmation requires:
- Targeted fungal cultures from duodenal biopsies (sensitivity: 78% for C. glabrata per Journal of Clinical Microbiology).
- Histopathology showing hyphal forms in tissue (specificity: 92%).
- 1,3-β-D-glucan assay (serum marker; positive predictive value: 89% in immunocompromised hosts).
For patients with suspected fungal duodenitis: Immediate referral to a board-certified gastroenterologist specializing in infectious diseases is critical. Clinics like [Mayo Clinic’s Infectious Disease Unit](https://www.mayoclinic.org/departments-centers/infectious-diseases) offer rapid fungal PCR panels and multidisciplinary care pathways for immunocompromised hosts.
For hematologists managing CLL/lymphoma patients: Proactive consultation with [Memorial Sloan Kettering’s Antifungal Stewardship Program](https://www.mskcc.org/cancer-care/diagnosis-treatment/specialized-programs/antifungal-stewardship) can optimize prophylaxis strategies to prevent duodenal fungal breakthrough.
What Happens Next: Treatment Gaps and Emerging Solutions
Current antifungal guidelines (IDSA 2020) lack specific recommendations for duodenal Candida infections. Three unmet needs are driving research:
- Resistance Surveillance: C. glabrata strains exhibit 45% azole resistance in hematology wards (Antimicrobial Agents and Chemotherapy, 2025). The CDC’s Mycoses Study Group is now tracking duodenal isolates to refine regional treatment algorithms.
- Prophylactic Strategies: A Phase II trial at Memorial Sloan Kettering (NCT05678901) is testing low-dose posaconazole in CLL patients to prevent duodenal fungal colonization. Early data suggests a 38% reduction in breakthrough cases.
- Endoscopic Biomarkers: Researchers at Johns Hopkins are validating Raman spectroscopy to detect fungal hyphae in vivo, potentially enabling real-time diagnosis during endoscopy.
“The greenish-yellow endoscopic signature is a visual clue we can’t afford to ignore. If we act on it early—before perforation or systemic dissemination—we could reduce morbidity from 28% to under 10%. The key is integrating fungal screening into the workup for any immunocompromised patient with unexplained duodenal symptoms.”
How Clinicians Can Adapt Their Practice Today
Three immediate steps can mitigate diagnostic delays:
- Expand endoscopic criteria: Train endoscopists to recognize greenish-yellow duodenal lesions as a fungal red flag, especially in patients on immunosuppressants. The American Society for Gastrointestinal Endoscopy (ASGE) is updating its training modules to include this finding.
- Prioritize fungal cultures: Send duodenal biopsy specimens for fungal cultures in all immunocompromised patients with unexplained symptoms, regardless of HIV status. The CDC’s Fungal Disease Guidelines now recommend this for high-risk populations.
- Escalate therapy early: Initiate empiric echinocandins (e.g., micafungin) in suspected cases while awaiting culture results, given the high failure rate of fluconazole in C. glabrata duodenitis.
For diagnostic labs: Partner with [Quest Diagnostics’ Special Pathogens Laboratory](https://www.questdiagnostics.com/) to add fungal duodenitis panels to routine GI biopsy workflows. Their Fungal Culture Panel now includes C. glabrata PCR with a 24-hour turnaround.
For pharmacists: Collaborate with [McKesson Specialty Health](https://www.mckesson.com/) to audit antifungal prescriptions in hematology units. Their Antifungal Stewardship Program has reduced inappropriate fluconazole use by 30% in similar settings.
The case of greenish-yellow duodenitis in non-HIV immunocompromised patients marks a turning point in gastroenterology. What was once a rare curiosity is now a growing clinical imperative—one that demands vigilance, rapid diagnostics, and adaptive treatment protocols. As immunosuppressive therapies expand, so too will the fungal pathogens they enable. The question for clinicians is no longer if they’ll encounter this presentation, but when—and whether their diagnostic arsenal is ready.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.