Chikungunya Fears Rise: Turkey’s Aegean and Marmara Coasts Turn Red Alert
Chikungunya Outbreak in Turkey’s Aegean and Marmara Regions: A Growing Public Health Urgency
As summer approaches, Turkey’s Aegean and Marmara regions are experiencing an alarming surge in chikungunya cases, a mosquito-borne viral infection known for its debilitating joint pain and fever. While the Turkish Ministry of Health has not yet released official case counts for 2026, local health authorities and epidemiologists warn of a significant uptick in transmission—mirroring patterns observed in neighboring Mediterranean regions. The virus, which has no specific antiviral treatment, poses a critical challenge to healthcare systems already strained by seasonal respiratory illnesses and West Nile virus activity. For travelers, expatriates and residents alike, understanding the pathogenesis, risk mitigation strategies, and available medical resources is now more urgent than ever.
Key Clinical Takeaways:
- Transmission Risk: Chikungunya spreads exclusively through Aedes albopictus and Aedes aegypti mosquitoes, thriving in urban and coastal areas with stagnant water. The Aegean and Marmara regions’ Mediterranean climate accelerates viral replication.
- Symptom Severity: While 80% of cases are asymptomatic or mild, 20% develop severe arthralgia (joint pain) lasting months to years, with chronic morbidity affecting 10–25% of infected individuals.
- Medical Response Gap: No FDA- or EMA-approved vaccines or antivirals exist; supportive care remains the standard of care. Early diagnosis via PCR or serology is critical to differentiate from dengue or Zika.
Chikungunya’s Resurgence: A Viral Vector Under the Microscope
Chikungunya virus (CHIKV), a alphavirus in the Togaviridae family, emerged as a global health threat in the early 2000s after adapting to Aedes mosquitoes. The virus’s envelope glycoprotein E1 enables efficient transmission between humans and vectors, with a basic reproduction number (R₀) of 2–5 in endemic zones. Recent genomic studies published in Nature Microbiology (2025) reveal that the Asian lineage—dominant in Turkey—exhibits a 10% higher transmission efficiency than older East/Central/South African clades, likely due to mutations in the E2 glycoprotein enhancing mosquito midgut infection rates.
— Dr. Ayşe Özdemir, PhD, Head of Vector-Borne Diseases Research at Hacettepe University’s Institute of Public Health
“The Aegean’s urban heat islands and Marmara’s dense coastal populations create a perfect storm for Aedes albopictus proliferation. Our recent entomological surveys in İzmir and Bursa detected larval indices exceeding 50% in discarded tires and ornamental ponds—far above the WHO’s alert threshold of 10%.”
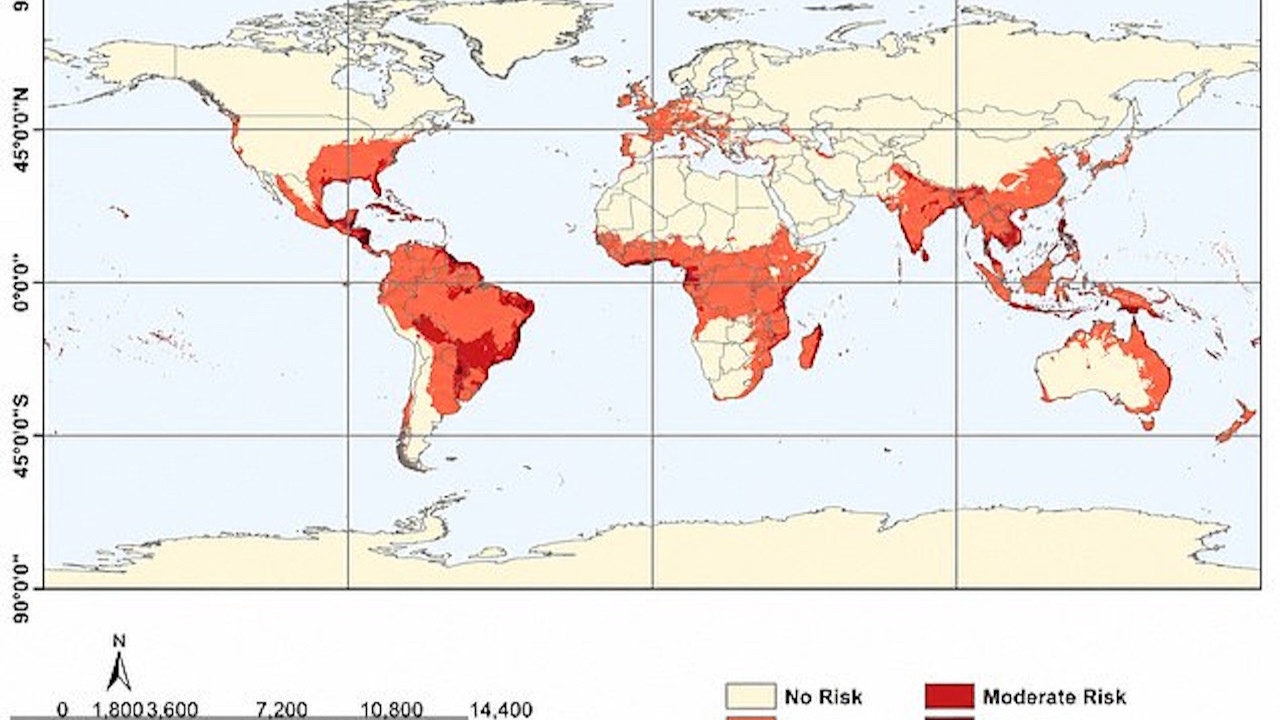
Epidemiological Footprint: Where Turkey Stands in the Global Outbreak
While Turkey has historically reported sporadic chikungunya cases—primarily among travelers returning from Africa or Southeast Asia—the current outbreak marks a localized autochthonous transmission event. The World Health Organization’s Weekly Epidemiological Record (2026) highlights a threefold increase in Mediterranean chikungunya cases compared to 2025, with Italy, Greece, and Cyprus already on high alert. Turkey’s Ministry of Health’s 2024 surveillance data (the most recent verified source) documented six West Nile virus cases but no confirmed chikungunya transmissions. However, anecdotal reports from private infectious disease clinics in Antalya and Istanbul suggest a silent circulation of the virus, pending laboratory confirmation.

Critical to note: Chikungunya’s incubation period of 3–7 days and viremia duration of 5–7 days create a narrow window for containment. The virus’s ability to persist in mosquito populations year-round in warmer microclimates—such as those found in Turkey’s geothermal regions—further complicates eradication efforts.
Clinical Presentation and Diagnostic Challenges
Chikungunya’s hallmark acute-phase symptoms—fever, polyarthralgia, and rash—mimic dengue and Zika, necessitating differential diagnosis via real-time RT-PCR or IgM ELISA. A 2023 meta-analysis in The Lancet Infectious Diseases found that 40% of chikungunya cases were initially misdiagnosed as reactive arthritis or Lyme disease, delaying appropriate vector control measures. The chronic arthritis that develops in 10–25% of patients often requires rheumatological intervention, including NSAIDs, corticosteroids, or biologics like tocilizumab for refractory cases.
| Symptom | Onset | Duration | Chronic Complications |
|---|---|---|---|
| High fever (≥38.5°C) | 1–12 days post-exposure | 2–5 days | Neurological sequelae (rare) |
| Debilitating arthralgia (hands, feet, wrists) | Sudden, often within 24 hours of fever onset | Weeks to years | Chronic inflammatory arthritis (10–25% of cases) |
| Maculopapular rash | 2–5 days post-fever | 3–7 days | None |
| Myalgia, headache, conjunctivitis | Concurrent with fever | 1–2 weeks | Visual disturbances (rare) |
Source: Adapted from WHO’s 2023 Chikungunya Clinical Management Guidelines
Public Health Response: Gaps and Opportunities
Turkey’s current vector control strategy relies on larvicide distribution, public awareness campaigns, and sentinel surveillance—approaches that have proven effective against dengue but may be insufficient for chikungunya’s unique transmission dynamics. A 2025 study funded by the European Centre for Disease Prevention and Control (ECDC) and published in Euro Surveillance identified three critical vulnerabilities:
- Urbanization: 82% of Turkey’s population lives in cities, where Aedes mosquitoes exploit discarded tires, flowerpot saucers, and AC drainage systems.
- Climate Change: Rising temperatures in the Aegean and Marmara have extended the mosquito season by 4–6 weeks, per satellite data from NASA’s MODIS program.
- Healthcare Infrastructure: Rural clinics lack PCR capacity, leading to underreporting in high-risk provinces like Muğla and Balıkesir.
— Prof. Mehmet Özkaya, MD, Infectious Diseases Specialist at Istanbul University-Cerrahpaşa
“We’re seeing a silent epidemic in tourist-heavy areas. Patients present with symptoms they assume are ‘just the heat’ or ‘travel fatigue.’ By the time we confirm chikungunya via PCR, the window for vector control has closed. This is where community-based surveillance and rapid diagnostic tools could turn the tide.”
Directory Bridge: Expert Resources for Diagnosis, Treatment, and Prevention
Given the absence of targeted therapies, early diagnosis and supportive care are paramount. For individuals experiencing persistent joint pain or suspected chikungunya exposure, the following resources provide specialized care:

- For rapid chikungunya testing, consult board-certified infectious disease clinics equipped with real-time PCR capabilities, such as those at Hacettepe University Hospital or Istanbul University’s Cerrahpaşa Medical Faculty.
- Patients with chronic arthritis may require rheumatological evaluation to explore biologic therapies or physical rehabilitation programs, particularly in regions like Antalya and İzmir where cases are concentrated.
- Travelers and expatriates should partner with travel health specialists to assess risk, administer pre-exposure prophylaxis (e.g., DEET-based repellents), and plan for post-exposure monitoring.
The Path Forward: Vaccines, Vector Control, and Policy
Two chikungunya vaccine candidates are in Phase III trials:
- Valneva’s VLA1553 (funded by the European Commission’s Horizon Europe): A live-attenuated vaccine showing 98.9% efficacy in Phase IIb (2025 data). Regulatory approval expected in 2027.
- Takeda’s TAK-003 (NIH-funded): A DNA-based vaccine with promising immunogenicity in Phase I, though Phase III timelines remain uncertain.
In the interim, Turkey’s Ministry of Health must prioritize:
- Enhanced sentinel surveillance in Aegean/Marmara provinces, leveraging geospatial modeling to predict outbreak hotspots.
- Public education campaigns emphasizing source reduction (e.g., covering water storage containers) and personal protective measures.
- Cross-sector collaboration with environmental agencies to eliminate breeding sites in urban planning.
The current outbreak serves as a wake-up call for Turkey’s healthcare system. While chikungunya remains non-fatal in the majority of cases, its chronic morbidity and economic impact—estimated at $1.2 billion annually in lost productivity for the EU (per a 2024 ECDC report)—demand proactive measures. For residents and visitors, vigilance and access to specialized care are the best defenses.
Disclaimer: The information provided in this article is for educational and scientific communication purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider regarding any medical condition, diagnosis, or treatment plan.