
Glaucoma Surgery Advances: A Step-by-Step Guide for Cataract Surgeons
CLEVELAND,OH – A growing opportunity exists for cataract surgeons to expand their practise to include microinvasive glaucoma surgery (MIGS),offering patients a potential path to reduced medication dependence and improved glaucoma control. A recent guide details the essential steps for incorporating MIGS into a surgical workflow, emphasizing that the procedures are accessible to those already proficient in cataract surgery.
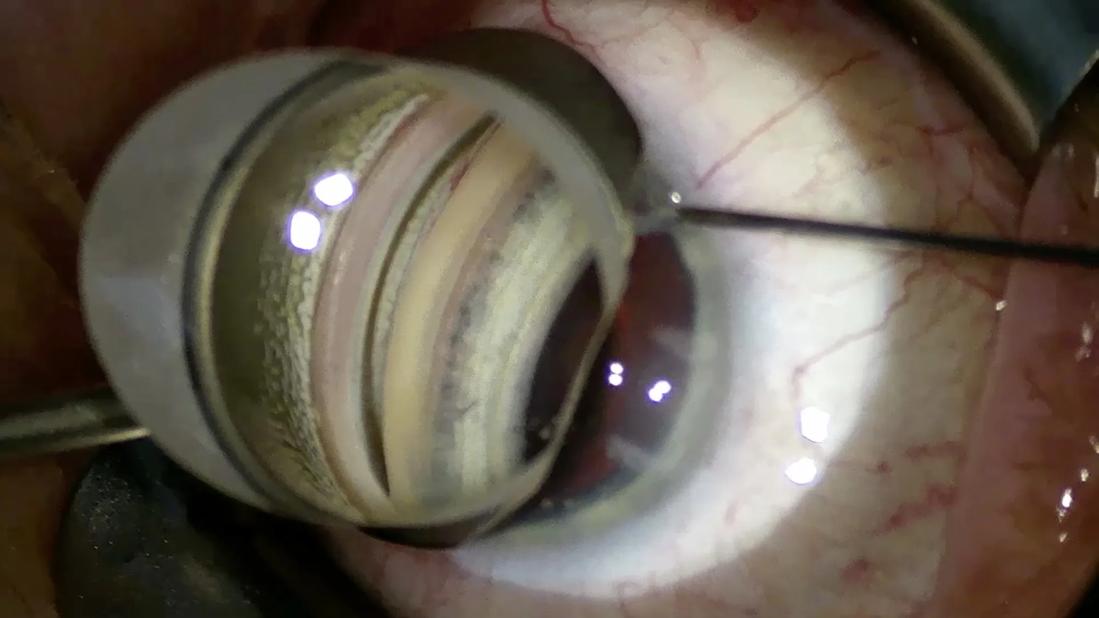
The process begins with meticulous preparation for gonioscopy, a critical skill for visualizing the angle structures. This involves utilizing a gonioprism – either a Goldmann, posner, or Goniosol – and ensuring optimal corneal coupling with viscoelastic.
Successful MIGS relies heavily on proper positioning. Surgeons are advised to tilt the patient’s head 45 degrees away from themselves, lower the chair, adjust microscope oculars upwards, re-zero the scope, and rotate it 30 degrees away. magnification is typically increased beyond that used for standard cataract surgery, focusing on the angle structures extending to the limbus.Depression with a stabilizer, if a hands-free prism isn’t used, can aid visualization, but excessive pressure on the cornea should be avoided to prevent viscoelastic egress.
Postoperative care is equally notable. Patching the eye until the first postoperative day is recommended, alongside strong steroid and NSAID drops to manage inflammation. A dexamethasone ophthalmic insert (like Dextenza®) can be considered as needed. Prostaglandin drops might potentially be temporarily discontinued to minimize the risk of cystoid macular edema. IOP management postoperatively depends on the severity of glaucoma; mild, well-controlled POAG or low IOP may allow for discontinuation of all drops, while more severe cases or higher IOPs necessitate non-prostaglandin alternatives like brimonidine timolol or dorzolamide timolol, particularly in the presence of hyphema.
The guide stresses the accessibility of MIGS for cataract surgeons: “If you can do cataract surgery,you can do MIGS.” Offering MIGS to glaucoma patients undergoing cataract surgery is encouraged due to its minimal additional risk and surgical time. It presents a valuable opportunity to reduce or eliminate the need for eye drops, improving patient lifestyle and reducing financial burden, and possibly better controlling glaucoma, though future procedures may still be necessary.
For surgeons seeking further knowledge, a companion piece, “How to Get Started with Microinvasive Glaucoma Surgery (Part 2),” provides a primer on specific MIGS methods and devices.
Drs.Bajic and Markakis of Cleveland Clinic cole Eye Institute authored the guide, advocating for patient access to MIGS through referral when surgeons are not yet comfortable performing the procedures themselves.